Download
1 / 67
670 likes | 878 Views
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease. Prof. Mohamed Sobhy, MD, FACC Professor of Cardiology, Alex. University Fellow of American College of Cardiology. International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease.

E N D
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease Prof. Mohamed Sobhy, MD, FACCProfessor of Cardiology, Alex. UniversityFellow of American College of Cardiology
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease • Definition of guidelines. • Rationale and objectives of guidelines. • What are the international guidelines for prevention of atherosclerotic CVD • Total CV risk as a guide to preventive strategies. • Management of CV risk as a guide to preventive strategies • Importance of Egyptian guidelines. • Public health Challenges and Community programs. • Prevention programs.
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease • Definition of guidelines. • Rationale and objectives of guidelines. • What are the international guidelines for prevention of atherosclerotic CVD • Total CV risk as a guide to preventive strategies. • Management of CV risk as a guide to preventive strategies • Importance of Egyptian guidelines. • Public health Challenges and Community programs. • Prevention programs.
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease • Guidelines: • Aim to present all the relevant evidence on a particular issue in order to help physicians to weigh the benefits and risks of a particular diagnostic or therapeutic procedure. • They should be helpful in everyday clinical decision-making.
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease • Definition of guidelines. • Rationale and objectives of guidelines. • What are the international guidelines for prevention of atherosclerotic CVD • Total CV risk as a guide to preventive strategies. • Management of CV risk as a guide to preventive strategies • Importance of Egyptian guidelines. • Prevention programs. • Public health Challenges and Community programs.
The Rationale for an active approach to the prevention of cardiovascular diseases (CVD) is firmly based on five observations: • CVD is the major cause of premature death in most populations; it is an important source of disability and contributes in large part to the escalating costs of health care • the underlying pathology is usually atherosclerosis, which develops insidiously over many years and is usually advanced by the time symptoms occur • death, myocardial infarction and stroke nevertheless frequently occur suddenly and before medical care is available, and many therapeutic interventions are therefore inapplicable or palliative • the mass occurrence of CVD relates strongly to lifestyles and modifiable physiological factors • risk factor modifications have been unequivocally shown to reduce mortality and morbidity, especially in people with either unrecognized or recognized CVD.
Objectives of Cardiovascular Prevention • To reduce the incidence of first or recurrent clinical events due to coronary heart disease, ischemic stroke and peripheral artery disease. • The focus is prevention of disability and early death. • Lifestyle changes, management of major CV factors, use of different prophylactic drug therapies. • Intermediate end-points… subclinical organ damage [LVH, CA plaque, ED, electrical instability]
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease • Definition of guidelines. • Rationale and objectives of guidelines. • What are the international guidelines for prevention of atherosclerotic CVD • Total CV risk as a guide to preventive strategies. • Management of CV risk as a guide to preventive strategies • Importance of Egyptian guidelines. • Public health Challenges and Community programs. • Prevention programs.
Recent international guidelines • American College of Cardiology (ACC) 2001 update • American Heart Association (AHA) 2002 update • CANADIAN Cardiovascular Society 1998 Consensus. • International Task Force for prevention of Coronary heart disease • Joint British recommendation for prevention of CHD 2002 • European guidelines on CVD prevention in clinical practice 2003
Recent international guidelines • American College of Cardiology (ACC) 2001 update • American Heart Association (AHA) 2002 update • CANADIAN Cardiovascular Society 1998 Consensus. • International Task Force for prevention of Coronary heart disease • Joint British recommendation for prevention of CHD 2002 • European guidelines on CVD prevention in clinical practice 2003
Recent international guidelines • American College of Cardiology (ACC) 2001 update • American Heart Association (AHA) 2002 update • CANADIAN Cardiovascular Society 1998 Consensus. • International Task Force for prevention of Coronary heart disease • Joint British recommendation for prevention of CHD 2002 • European guidelines on CVD prevention in clinical practice 2003
Recent international guidelines • American College of Cardiology (ACC) 2001 update • American Heart Association (AHA) 2002 update • CANADIAN Cardiovascular Society 1998 Consensus. • International Task Force for prevention of Coronary heart disease • Joint British recommendation for prevention of CHD 2002 • European guidelines on CVD prevention in clinical practice 2003
Canadian Cardiovascular Society 1998 Consensus Conference On The Prevention Of Cardiovascular Diseases:The Role Of The cardiovascular Specialist
Recommendations for assessment with fasting lipid profile (total cholesterol, high density lipoprotein cholesterol, triglyceride and low density lipoprotein levels) in various patient groups Clinical judgement should be used for patients with multiple risk factors who are approaching these target ages. Note that the translation of number of risk factors into risk levels is incorrect outside of these age ranges. CAD Coronary artery disease
Recent international guidelines • American College of Cardiology (ACC) 2001 update • American Heart Association (AHA) 2002 update • CANADIAN Cardiovascular Society 1998 Consensus. • International Task Force for prevention of Coronary heart disease • Joint British recommendation for prevention of CHD 2002 • European guidelines on CVD prevention in clinical practice 2003
Recent international guidelines • American College of Cardiology (ACC) 2001 update • American Heart Association (AHA) 2002 update • CANADIAN Cardiovascular Society 1998 Consensus. • International Task Force for prevention of Coronary heart disease • Joint British recommendation for prevention of CHD 2002 • European guidelines on CVD prevention in clinical practice 2003
EditorialNew British recommendations for prevention of coronary heart disease in clinical practice Heart 1999; 81:335 (April)
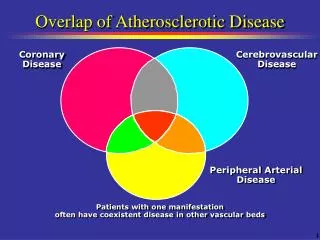
Priorities for CHD prevention in clinical Practice • A. Patients with established CHD.B. Patients with other major atherosclerotic disease. • Patients with HTN, dyslipidemia, DM, FH of premature CHD or combination.
Using the coronary risk prediction chart for primary prevention • Charts are not appropriate for: • Coronary Heart Disease or other major atherosclerotic disease. • Familial hypercholeserolemia or other inherited dyslipidemia • Established hypertension (Systolic >160mmHg or diastolic > 100mmHg or associated TOD) • DM with associated TOD • Renal dysfunction
People at high risk without clinically overt CHD or other major atherosclerotic disease • Patients with HTN, dyslipidemia, diabetes mellitus, FH of premature CHD or combination are at high risk of developing CHD • Patients with DM are at particularly high risk • Individuals at high multifactorial risk of developing CHD or other atherosclerotic disease • As absolute risk of coronary heart disease increases, so lifestyle intervention should be intensified
New British recommendations for prevention of coronary heart disease in clinical practice • The joint British recommendations on prevention of coronary heart disease in clinical practice closely mirror the European guidelines. • The difference reflect intelligent adaptations to national conditions and concerns • The recommendations concerning primary prevention are based on the assessment of risk, in absolute terms of developing clinical coronary disease within the next year
The assessment is based on • Framingham risk function (age, sex, smoking status, SBP, lipids measurements) • British recommend ratio of total HDL • Level of risk at which to intervene in primary prevention • European recommends 10 year risk of CHD 20% • British a staged approach • High risk >30% • Low risk 15%
BP …. Based on BP alone rather than BP in the context of absolute CV risk. • British recommendations: • BP>160/110 mmHg should be lowered irrespective of other factors because of established benefit in reducing the cerebrovascular component of CV risk • 15% risk of CHD corresponds to 20% overall CV risk. • In persons of BP 140-160/90-100 mmHg. British Society starts treatment when risk of CAD >15%
Introducing drug treatment for raised BP or lipid concentration should be strongly determined by the absolute risk of developing disease. • An absolute risk of coronary heart disease >15% (equivalent to a CV risk of 20%) over 10 years is sufficiently high to justify drug treatment.
Exceptions to treatment based on absolute risk are: • Hypertension (SBP>160mmHg or diastolic BP>100mmHg) or HTN with associated target organ damage. • Familial hypercholestrolemia or other inherited dyslipidemia. • Diabetes Mellitus with associated target organ damage. • Drug treatment is required for all these patients to reduce the risk of CHD (and CV risk).
A staged approach to managing patients at high risk is advised. • As a minimum, those with absolute CHD risk >30% should be targeted and treated now. • As resources allow individuals with a risk >15% should be progressively targeted • For all high risk patients every effort should be made to achieve the lifestyle, risk factor and therapeutic targets.
Recent international guidelines • American College of Cardiology (ACC) 2001 update • American Heart Association (AHA) 2002 update • CANADIAN Cardiovascular Society 1998 Consensus. • International Task Force for prevention of Coronary heart disease • Joint British recommendation for prevention of CHD 2002 • European guidelines on CVD prevention in clinical practice 2003
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease • Definition of guidelines. • Rationale and objectives of guidelines. • What are the international guidelines for prevention of atherosclerotic CVD • Total CV risk as a guide to preventive strategies. • Management of CV risk as a guide to preventive strategies • Importance of Egyptian guidelines. • Public health Challenges and Community programs. • Prevention programs.
International Guidelines for Prevention of Atherosclerotic Cardiovascular Disease • Definition of guidelines. • Rationale and objectives of guidelines. • What are the international guidelines for prevention of atherosclerotic CVD • Total CV risk as a guide to preventive strategies. • Management of CV risk as a guide to preventive strategies • Importance of Egyptian guidelines. • Public health Challenges and Community programs. • Prevention programs.