Download
1 / 75
770 likes | 1.23k Views
Impact of Hospitalization. Chapter 1 C. Cummings, RN, EdD. What is Health?. How do you define health? Health-illness continuum Is it the ability of one to function in society? Is it disease free ? Health: free from disease/illness. Different for everyone.

E N D
Impact of Hospitalization Chapter 1 C. Cummings, RN, EdD
What is Health? • How do you define health? • Health-illness continuum • Is it the ability of one to function in society? • Is it disease free? • Health: free from disease/illness. Different for everyone. • Needs to be their goal for health, not ours.
WHO’s definition of health • State of complete physical, mental and social well-being • Is this realistic? • Holistic health- body, mind and spirit as part of a person’s level of wellness • (not really realistic)
Quality of Life • Quality of Life, refers to 2 concepts: • Subjectivity: perceptions of satisfaction with their functional level • Multidimensionality: physical, functional, emotional and social well-being
Health Promotion and Protection • Health Promotion: What is this? • Healthy people 2010: U.S. DHHS • 2 National Goals: • Increase quality and years of healthy life • Eliminate health disparities among demographic groups • Pender (1987) describes health promotion as a positive activity that protects someone against illness • DRG: diagnosis related group. If you are admitted to hospital… hospital can get a certain amt of money from Medicare for that diagnosis. Hospital has to get every thing that patient needs w/in that amount of money. Now, the patient will add more diagnosis so the patient is able to get more money. • Pender (nurse) has written a lot on health promotion
Activities to Promote Health • Name some activities to promote health • Why are the effective and why might they not be? • (exercise, smoking, diet, seat belt, stress relief activities, lower cholesterol, diabetes prevention)
Healthy People 2010 • http://www.healthypeople.gov/ • Look at leading health indicators. Gov says we have to go by these things! • Physical activity, overweight & obesity, tobacco use, substance abuse, resp sex behavior, mental health, injury & violence, environmental quality, immunization and access to health care.
Healthy People 2010 • What are the 6 target areas of health promotion? • Do you think there is a difference between racial and ethnic groups? • Yes, there is a difference w/ access to care, cultural differences w/ tobacco use or diet, communication issues…
Reasons for Differences • Poor Socioeconomic status • Health beliefs and behaviors • Access to health care • Environmental factors • Direct and indirect manifestations of discrimination • Lack of health insurance • Insufficient transportation • Geographic location • Cost of services • Language barriers • (transportation difficult here in Jax for elders)
Nursing’s Role • What can nurses do to decrease these differences? • What is transcultural nursing? • Area of study that focuses on the care, health and illness patterns as related to one’s cultural beliefs, values and practices • What is cultural competence? • Name some areas that may have differences for a hospitalized patient. • Being familiar w/ other cultures & groups… being aware, not putting our own prejudices & bias on them. • Getting patient to understand meds
Illness Prevention • People must be motivated to prevent an illness from occurring • What do you think motivates them? • What role can you as a nurse play? • The pt has to see it as a problem. Families may motivvate… hopefully as a nurse we motivate.
Three Types of Prevention • Primary Prevention: • Early, health maintenance activities • Secondary Prevention: • Early detection and treatment of a disease or condition (when the person has the disease) • Tertiary prevention: • Rehabilitation once the disease is stabilized • Return to their highest level of functioning
What types of Prevention are these? • Cardiac Rehab Program • Colonoscopy after 50 • Hepatitis B vaccine • Cholesterol testing • Asthma camp for children • Running with a group • Secondary is hardest to pick out… • Tertiary • Primary or secondary • Primary • Secondary • Tertiary • Primary
Impact of Hospitalization • What impact do you think being hospitalized has on someone? • List three nursing diagnoses related to hospitalization. • Communicate w/ patients about what is going on. • Allow patient to make choices about their care. Powerlessness is a huge problem.
Powerlessness • Ackley’s definition of powerlessness: • Perception that one’s own action will not significantly affect an outcome • Lack of control over the situation • How does being hospitalized contribute to this diagnosis? • (if you tell most patients why youaredoing something, they will cooperate)
Powerlessness • List some patient behaviors that may demonstrate this diagnosis • May be angry… may take the anger out on the nurse… may withdraw or be depressed… • NOC outcomes may be the following: • Health beliefs: Perceived control • Health beliefs: Perceived ability to preform • Participation in health care decisions • Depression level: self-control
Nursing Interventions • List 5 things that nurses can do to help the patient experiencing powerlessness • How can you empower a patient?
Hopelessness • Subjective state in which the person sees limited or no alternatives and is unable to mobilize any energy to correct • What do you see as the difference between hopelessness and powerlessness? • What patient behaviors may be different? • Get a family member in w/ them… Difference: powerlessness; you feel like you can get the control back. Hopelessness: watch for depression & suicidal behavior
Hopelessness • List 4 nursing interventions that may be helpful. • What should the nurse be aware of, if the patient is exhibiting hopelessness? • Talk to them, keep them involved, talk about experiences… long term, be honest but tell that we will do everything we can
Role of the Nurse • What then is the role of the nurse in patient care? • Coordinator of Care • Caregiver • Continuing Care Planner: discharge • Educator • Advocate • Change Agent
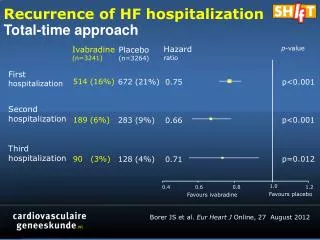
Theories of Chronic Illness • Chronic Illness • Condition or illness that has existed for more than 3 months • Chronic Disease accounts for 70% of all health care deaths and 60% of all health care costs • $510 billion in 2000 and may increase $2 trillion by 2020 • Over 125 million people have one or more chronic disease • Heart disease & cancer, numbers 1 & 2 • Chronic disease= more than 3 months
Uncertainty Modelfirst diagnosed: uncertain. Get more understanding over time
Model of Uncertainty in IllnessHow to adapt & cope. Inference Illusion (get info from web md & make an inference about what I think the heart disease is)
Chronic Illnesses • List the top 5 common chronic illnesses • 1. • 2. • 3. • 4. • 5. • What is the leading cause of death for those over 65?
Chronic Illnesses • http://www.cdc.gov/nchs/FASTATS/default.htm • http://www.ncsl.org/programs/health/phchronic.htm • CDC: leading cause of death: heart disease is number 1, cancer #2, stroke, chronic lower resp disease, accidents, diabetes, alzheimer’s disease, influenza & penumonia, renal syndromes, septicemia • Life expectancy: 77.7 years • death rate 940 per 100,000 • NCLS website: state information, website not up right now
Theories of Chronic Illness • Why are some patients more independent than others? • Some illnesses are less debilitating • Some are controlled by medications • Some have the resources to self-manage • Financial • Emotional
Theories of Chronic Illness • Shifting Perspectives • Shift between well and ill • Taking on the Sick Role • Finding meaning, hope and quality of life • Accepting or denying illness
Issues with the Chronically Ill • Education of RN’s about elderly and chronic illness • Only 12% of RN’s are from ethically diverse groups, while 33% of ill are from these groups • Financial issues • Medications, MD visits, home care and ADL’s • Cultural values • Not a priority for family support • Need more nurses from other cultures
Health Care Needs of the Aging Irma B. Ancheta, Ph. D, RN Peggy McCartt, RN, PhD (c), CCRN, ARNP
Learning Objectives • Identify the four subgroups of older adults • Discuss common health issues that may concern the older adult • Explain why older adults are at risk for falls • Discuss polypharmacy in the older adult • Discuss economic issues for older adults • Describe government and community resources for older adults
Four Subgroups of Older Adults • 65-74 years of age: young old • 75-84 years of age: middle old • 85-99 years of age: old old • 100 years of age or more: the elite old
Questions About These Groups • Which is the fastest growing of the four subgroups? • What percentage of older adults are living in the community either at home, in assisted-living, or in community retirement complexes? • Old old is the fastest growing • Almost 80% are living in the community. • Page 15 in the book
Health Issues for Older Adults • Health Promotion • Self-management • Nutritional Awareness • Physical Fitness and Mobility • Stress Management • Accidents • Drug Use and Misuse • Mental Health/Behavioral Health Problems • Elder Neglect and Abuse • (isolation, accidents, falls, leaving stove on, etc…)
Relocation Stress Syndrome • “physiological and /or psychological distress following transfer from one environment to another.” (NANDA, 2003) (transferring from one environment to another is very stressful for elderly… confusing)
Health Promotion Negative Risk Factors for Healthy Aging • Alcohol Abuse • Smoking • Depression • Lack of Exercise • Obesity
Health Promotion • Yearly Influenza Vaccinations • Pneumococcal Vaccination • Tetanus Immunization • Create Hazard Free Environment • Wear Seat Belts • Install Smoke Detectors • Be Cautious About Medication Use • Take One Aspirin a Day • Moderate Alcohol Intake • No Smoking
Self-management Find Opportunities to be productive Maintain as much control as possible over their lives Participate in decision making Perform as many tasks as possible (avoid being an enabler)
Nutritional Awareness • Increase Intake of Fiber and Complex Carbohydrates (add Benefiber in coffee) • Decrease Intake of Dietary Fat • Increase Calcium Intake (also need sunlight exposure)
Nutritional Awareness Causes of poor nutrition (not eating/ eating less or overeating) in the elderly: [1] Loneliness (PF) [2] Depression (SB) [3] Boredom ………………..lose the will to live……
Physical Fitness and Mobility Exercise Regularly (three to five times a week for 30 minutes per session) Some Weight Bearing Exercises (increase strength) Improve regularity of bowel movement
Physical Fitness and Mobility • Use of walker, cane, wheelchair, motorized scooter • Health and beauty trips
Stress Management • Older Adults Cope with Stress as they Did when they were Younger • Awareness of Physical and Economic Constraints • (get stressed that they can’t do what they used to be able to do…. Frustration)
Accidents • Most Accidents are at Home FALLS
Drug Use and Misuse • POLYPHARMACY • (occurs often due to elderly pt receiving a lot of different meds from different pharmacies)
Drug Use and Misuse Older people have less muscle mass….. …….inclined to get easily toxic to drugs… …….beware of how drugs affect the elderly Has more to do with liver involvement, bioavailability. Liver just not as effective. Can also be a renal problem w/ excretion. Statins are really rough on the liver (cholesterol lowering drugs). Tylenol is also rough on the liver.
Mental Health/Behavioral Health Problems • Legally Competent • Clinically Competent • Depression (…the need to be intellectually stimulated) • Dementia/Delirium
Depression Watch out for: [1] early morning insomnia [2] excessive daytime sleeping [3] poor appetite [4] unwillingness to participate in social and recreational activities Wake up at 3 am, don’t sleep well, sleep throughout the day but not good at night. Depression very common in the elderly.
Depression: Treatment [1] Drug therapy [2] Psychotherapy [3] Awareness of depression and eliminate possible causes.