Download
1 / 42
420 likes | 579 Views
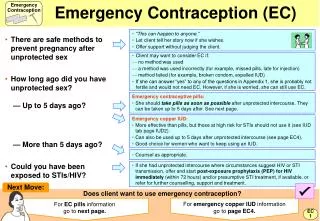
Clinical Issues in Emergency Contraception. James Trussell, PhD. Objective: To Enhance Understanding about These 7 Issues. New Plan B regimen Mechanism of action of ECPs Does EC promote risk taking? Are ECPs effective? Beginning contraception after ECPs When to expect menses after ECPs

E N D
Clinical Issues in Emergency Contraception James Trussell, PhD
Objective: To Enhance Understanding about These 7 Issues • New Plan B regimen • Mechanism of action of ECPs • Does EC promote risk taking? • Are ECPs effective? • Beginning contraception after ECPs • When to expect menses after ECPs • Enhancing availability of EC
New Plan B Regimen • Two studies have shown that both doses of Plan B (both Plan B pills) can be taken at the same time • With no reduction in effectiveness • With no increase in side effects • One study has shown that two doses of Plan B taken 24 hours apart are just as effective as two doses taken 12 hours apart • Two studies have shown that Plan B is effective up to 120 hours after intercourse Sources: Arowojoluet al. 2002; von Hertzen et al. 2002; Ngai et al. 2004
How MIGHT EC Work? • Inhibitovulation • Trap sperm in thickened cervical mucus • Inhibit tubal transport of egg or sperm • Interfere with fertilization, early cell division, or transport of embryo • Preventimplantationby disrupting the uterine lining
Mechanism of Action: LNg ECPs • Clinical evidence about the effect of progestin-only ECPs on ovulation, on uterine lining characteristics, and on timing of the next menstrual period • Observed vs. expected pregnancies by timing of administration relative to ovulation • One published study of effect of small doses of LNg on sperm motility Source: Kesseru et al. 1974; Durand et al. 2001;Croxatto et al. 2001;Hapangama et al. 2001; Marions et al. 2002; Croxatto et al. 2003; Marions et al. 2004; Croxotto et al. 2004; Durand et al. 2005; Novikova et al. 2007
Clinical Evidence: Progestin-only ECPs • Progestin-only ECPs can inhibit ovulation but do not always do so. Inhibiting ovulation may be the only mechanism of action. • Progestin-only ECPs may immobilize sperm by altering uterine pH. • Progestin-only ECPs can alter glycodelin in serum and endometrium and can shorten the luteal phase. Source: Kesseru et al. 1974; Durand et al. 2001;Croxatto et al. 2001;Hapangama et al. 2001; Marions et al. 2002; Croxatto et al. 2003; Marions et al. 2004; Croxotto et al. 2004; Durand et al. 2005; Novikova et al. 2007
Animal Evidence: Levonorgestrel • Studies in the rat and in the new-world monkey Cebus apella • Levonorgestrel administered in doses that inhibit ovulation has no postfertilization effect that impairs fertility Source: Müller et al. 2003; Ortiz et al. 2004
Mechanism of Action of Hormonal Contraceptives and IUDs About the same amount of evidence for each of the following statements: • ECPs, • OCs, implants, patches, rings, injectables, • IUDs, • The contraceptive effect of breastfeeding… MAY work by inhibiting implantation of a fertilized egg Source: ACOG 1998; Díaz et al. 1992
What Should Women Be Told? • ECPs—like all regular hormonal contraceptives such as the birth control pill, the implant Implanon, the vaginal ring NuvaRing, the Evra patch, and the injectable Depo-Provera, and even breastfeeding—may prevent pregnancy by delaying or inhibiting ovulation, inhibiting fertilization, or inhibiting implantation of a fertilized egg. • The best available evidence is consistent with the hypothesis that Plan B’s ability to prevent pregnancy can be fully accounted for by mechanisms that do not involve interference with post-fertilization events.. Source: Davidoff and Trussell 2006
Does Providing ECPs Increase Risk Taking? • Empirical evidence from 1 study in Scotland, 3 in San Francisco, 1 in Pittsburgh, 1 in Hong Kong, 1 in China, 2 in Los Angeles, and 1 in Nevada & North Carolina where women were randomized to receive counseling and ECPs on demand or to receive ECPs in advance for later use should the need arise. Source: Glasier and Baird 1998; Raine et al. 2000; Jackson et al. 2003; Gold et al. 2004; Lo et al. 2004; Raine et al. 2005; Hu et al. 2005; Belzer et al. 2005; Trussell et al. 2006; Raymond et al. 2006; Walsh et al. 2006
Results Scotland: Women who received ECPs in advance • Weremore likely to use ECPs: 47% vs 27% of women who received only counseling (p<.001) • Werenotmore likely to use ECPsrepeatedly • Used other methods of contraception equally well • Had fewer unintended pregnancies:3.3% vs 4.8 %for women who received only counseling (p=0.14) Source: Glasier and Baird 1998
Results San Francisco 1: Women who received ECPs in advance • Weremore likely to use ECPs: 22% vs 7% of women who received only counseling (p=.006) • Werenotmore likely to haveunprotected sex • Were not less likely to use condoms consistently • Were less likely to use oral contraceptives consistently: 32% vs 58% of women who received only counseling (p=.03) Source: Raine et al. 2000
Results San Francisco 2: Women who received ECPs in advance • Weremore likely to use ECPs: 17% vs 4% of women who received only counseling (p=.006) • Werenotmore likely to change to a less effective method of contraception • Were not more likely to have unprotected sex • Were not more likely to use contraception less consistently • Had fewer unintended pregnancies:7% vs 10%for women who received only counseling (p=0.16) Source: Jackson et al. 2003
Results Pittsburgh: Women who received ECPs in advance • Weremore likely to use ECPs: 15% vs 8% of women who received only counseling (p=.05) • Took ECPs sooner after sex (11 vs 22 hours) • Were more likely to use condoms • Were not less likely to use hormonal contraception Source: Gold et al. 2004
Results Hong Kong: Women who received ECPs in advance • Weremore likely to use ECPs: 30% vs 13% of women who received only counseling (p<.001) • Werenotless likely to use contraception consistently • Were notless likely to use condoms • Took ECPs sooner after sex (14 vs 29 hours) • Were not less likely to become pregnant Source: Lo et al. 2004
Results San Francisco 3: Women who received ECPs in advance • Weremore likely to use ECPs: 37% vs 21% of women who received only counseling (p<.001)) • Werenotmore likely to haveunprotected sex • Were notless likely to use condoms or pills consistently • Were not more likely to acquire an STI • Were not less likely to become pregnant Source: Raine et al. 2005
Results San Francisco 3: Women who received ECPs from a pharmacist • Wereno more likely to use ECPs: 24% vs 21% of women who received only counseling (p=.25) • Werenotmore likely to haveunprotected sex • Were notless likely to use condoms or pills consistently • Were not more likely to acquire an STI • Were not less likely to become pregnant Source: Raine et al. 2005
Results China: Women who received ECPs in advance • Weretwice as likely to use ECPs Werenotless likely to use contraception • Were notless likely to use condoms • Were not less likely to become pregnant Source: Hu et al. 2005
Results Los Angeles 1:Women who received ECPs in advance • Weremore likely to use ECPs: 83% vs 11% of women at 6 months and 64% vs 17% of women at 12 months who received only counseling (p<.01) • Were not more likely to have unprotected sex • Were not less likely to use condoms • Were not less likely to become pregnant Source: Belzer et al. 2005; Trussell et al. 2006
Results Los Angeles 2: Women who received ECPs in advance • Weremore likely to use ECPs: 19% vs 12% of women who received only counseling (p<0.05) • Werenotmore likely to haveunprotected sex • Were notless likely to use barrier methods or pills • Were not less likely to become pregnant Source: Walsh and Frezieres 2006
Results Nevada & North Carolina: Women who received ECPs in advance • Weremore likely to use ECPs: 71% vs 32% of women who received only counseling (p<0.001) • Werenotmore likely to haveunprotected sex • Were notless likely to use condoms or pills • Were not more likely to acquire an STI • Were not less likely to become pregnant Source: Raymond et al. 2006
Are ECPs Effective? • Eight of the ten studies conducted to test whether easy assess to ECPs increased risk taking also measured pregnancies • In none of the eight did advance provision of ECPs reduce pregnancy rates • Only three studies powered to detect a decrease in pregnancy rates Raymond et al. 2007
Why No Reduction in Pregnancies? • In San Francisco almost half of the women in the advance provision group who had unprotected intercourse did not use ECPs • In China, 30 of the 38 pregnancies in the advance provision group occurred to women who did not use ECPs in that cycle • In Nevada/NC, 57 of the 74 pregnancies in the advance provision group occurred to women who did not use ECPs in that cycle • Lesson: ECPs are not used frequently enough! Source: Raine et al. 2005; Hu et al. 2005; Raymond et al. 2006
Advance Provision of ECPs Did Not Reduce Abortions Rates in Lothian • Community intervention study in Scotland • About 1 in 5 women aged 16-29 got ECPs in advance to take home • About half of these used ECPs at least once • No effect on abortion rates was observed • Women most at risk probably did not get ECPs • 78% of women with advance supplies who got pregnant did not use ECPs. Source: Glasier et al. 2004
Excellent Evidence that Plan B Works • Two trials in which women were randomly assigned to Plan B or Yuzpe regimen. • Pregnancy rate in Plan B arm was 51% of the rate in the Yuzpe arm. • Plan B is 49% effective if Yuzpe regimen is completely ineffective. • If, for example, Yuzpe regimen is 60% effective, then Plan B is 79% effective. Source: Raymond et al. 2004
Effectiveness of LNg Excellent Evidence that Plan B Works Source: Raymond et al. 2004
Lessons Learned • ECPs are not used nearly frequently enough! • Women underestimate their risk of pregnancy • More education is needed • OTC switch is necessary―but not sufficient―for solving this problem • Major public health impact is unlikely
Beginning Contraception after EC • Oral contraceptives, patches, and vaginal rings, and injectables • Regular start: use backup until next period, then begin new method according to regular patient instructions • Jump/quick start: take 2 ECP doses. Start new method the next/same day (use backup for first seven days)
Initiating Ongoing Method: • Condoms immediately • Spermicides immediately • Diaphragm immediately • Implant within 7 days after next menses * • Mirena after next menses ** backup until menses
Bleeding Patterns After Plan B • Two studies specifically designed to assess the effects of ECPs containing 1.5 mg levonorgestrel taken in a single dose on bleeding patterns Source: Raymond et al. 2006; Gainer et al. 2006
Bleeding Patterns After Plan B―1 • The first study found that when taken in the first three weeks of the menstrual cycle, ECPs significantly shortened that cycle compared both to the usual cycle length and to the cycle duration in a comparison group of similar women who had not taken ECPs. The magnitude of this effect was greater the earlier the pills were taken. Source: Raymond et al. 2006
Bleeding Patterns After Plan B―1 • This regimen taken later in the cycle had no effect on cycle length, but it did cause prolongation of the next menstrual period • The ECPs had no effect on the duration of the post-treatment menstrual cycle, but the second period was prolonged • Intermenstrual bleeding was uncommon after ECP use, although more common than among women who had not taken ECPs Source: Raymond et al. 2006
Bleeding Patterns After Plan B―2 • The second study compared the baseline cycle with the treatment and post-treatment cycles. Cycle length was significantly shortened by one day when ECPs were taken in the preovulatory phase of the cycle and was significantly lengthened by two days when ECPs were taken in the postovulatory phase. No difference in cycle length was observed for women who took ECPs during the periovulatory phase of the cycle (from two days before to two days after the expected day of ovulation). Source: Gainer et al. 2006
Bleeding Patterns After Plan B―2 • Menstrual period duration increased significantly when ECPs were taken in the periovulatory or postovulatory phase in both the treatment and post-treatment cycles. • The duration of the post-treatment menstrual cycle remained significantly longer when ECPs were taken in the postovulatory phase. • During the treatment cycle, 15% of women experienced intermenstrual bleeding; this was significantly more common when ECPs were taken in the preovulatory phase Source: Gainer et al. 2006
EC Hotline and Website • Emergency Contraception Hotline • 1-888-NOT-2-LATE • 630k calls since 1996 • Emergency Contraception Website • http://not-2-late.com • 3.2m visits since 1994
State Websites: Prescriptions Called In • Georgia: www.ecconnection.org • Illinois: www.plannedparenthoodchicago.com • Indiana: www.ppin.org/ecaccess/ecinfo.html • Maine: www.ppnne.org • Massachusetts: www.pplm.org • North Carolina: http://www.pphsinc.org/ec/ • Oregon: www.ppcw.org • South Carolina: http://www.pphsinc.org/ec/ • Vermont: www.ppnne.org • Washington: www.ppcw.org • West Virginia: http://www.pphsinc.org/ec/
Statewide Hotlines: Prescriptions Called In • Connecticut: 800-230-PLAN • Georgia: 877-ECPills • Illinois : 866-222-EC4U or 217-544-2744 • Maryland: 877-99-GO-4-EC • Massachusetts: 800-682-9218, 642-5665, 539-2378 • Michigan: 734-973-0710 • Minnesota: 612-625-4607 • Montana: 800-584-9911 • New Mexico: 505-272-9304 • New York: 585-271-9055 • North Carolina: 866-942-7762 • South Carolina: 800-230-PLAN • West Virginia: 800-230-PLAN • Wisconsin: 877-975-9858
States with Call-in Prescriptions 39% of women aged 15-44
Alaska California Hawaii Maine Massachusetts Montana New Hampshire New Mexico Vermont Washington Canada France United Kingdom Australia South Africa 33 other countries+5 OTC Emergency Contraception BTC ECPs are available directly from pharmacists without having first to get a prescription in: