Download
1 / 40
490 likes | 965 Views
Emergency contraception. Emergency Contraception. “Post exposure methods which prevent fertilisation and possibly implantation and hence the establishment of pregnancy.”. Usual scenario. 20 yr old woman requests the “morning after pill” for upsi 36 hours ago.

E N D
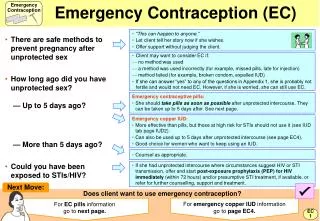
Emergency Contraception “Post exposure methods which prevent fertilisation and possibly implantation and hence the establishment of pregnancy.”
Usual scenario.... • 20 yr old woman requests the “morning after pill” for upsi 36 hours ago. • When you offer her a copper intrauterine device, ulipristal acetate or levornogestrel she looks surprised and says “can’t I just have the pill I had last time”
3 methods • Copper IUD; can be used up to 5 days following first UPSI in cycle or within 5 days from the earliest estimated day of ovulation. • Effectiveness >99% at any time of cycle.
Levonorgestrel, LNG • Levonelle 1500; prescribed £5.20 • Levonelle one step; otc £25 cost to patient • A progesterone; single 1.5mg dose • Use 12-13 years • Licensed for use up to 72 hours after UPSI or contraceptive failure; may be used up to 120 hours ( off licence)
Ulipristal/UPA “ellaOne” • A selective progesterone receptor modulator; single dose 30 mg. • Licensed for use up to 120 hours after UPSI or contraceptive failure. • Cost £16.95
When is EC needed? • Missed cocp • Late POP ( >27 hrs for conventional POP,>36 hours for cerazette) • Condom not used/ condom accident • Late depo >14w since last injection • IUD removal, expulsion, lost threads • Enzyme inducing drugs and failure to use extra precautions
How does it work? • IUD; copper toxic to sperm and ovum; primarily inhibits fertilisation (and implantation) • LNG; interferes with ovulation by inhibiting LH surge • ellaOne; delays LH surge and has effect on follicular rupture; additional action
Levonorgestrel, levonelle • Inhibits ovulation only if given before the LH surge. • It has no effect if given after ovulation.
Ulipristal, EllaOne • Suppresses lead follicles when given just before ovulation, including during the LH surge. • It is unclear if it has any effect after ovulation
How effective is it? • IUD >99% effective • LNG up to 95% within 24 hrs • up to 85% within 25-48 hrs • up to 58% within 49-72 hrs • UPA at least as effective as LNG up to 120 hours
Evidence LNG v UPA • Glasier; meta-analysis ( Lancet 2010) • Looked at 2 randomised controlled trials • Authors concluded that the pregnancy rate with UPA was significantly lower at all time periods analysed up to 120 hours.
Case one • 22 year old Elaine has just started a new job. She attends your surgery on Tues am after bank holiday weekend. She got drunk at a party on the Thursday night and cannot remember using condom. She is requesting a “morning after pill” • What other information do you need?
Case one • She has a predictable 28 day cycle and her last period started 9 days ago. She has not had any other acts of upsi this cycle. • What treatment would you offer her?
Date of LMP; Time since UPSI Previous UPSI this cycle? EC used this cycle? Duration shortest "usual" cycle; Discussed oral method v IUD? Ongoing contraception discussed? Condoms offered if needed? Given leaflets for EC and larc's. Need STI screen? Advised PT in 3weeks if no period;
Risk of pregnancy • Risk is highest mid cycle( 5 days before and 1 day after ovulation) Risk is 20-30% • Rest of cycle; risk is around 10% but due to unpredictable nature of ovulation there is no point at which one could guarantee that pregnancy won’t occur. • Implantation is always at least 5 days after ovulation.
Case two • 18 year old girl, no regular contraception. Sunday pm, on call centre. Had sex last night, condom came off. LMP started 10 days ago. She has a regular cycle, but can be up to 3 days early. She is very keen to avoid pregnancy as she is going to university after her gap year and is going on a college field trip tomorrow. • What method do you feel would be most suitable for her?
Case two • This is a mid cycle event; most risky time but she is only 24 hours after the event. • In theory; LNG or UPA can be used • UPA may offer a slight advantage due to its additonal effect on ovulation.
What are the side effects of EC? • IUD; pain • LNG and UPA; nausea, headache, altered bleeding pattern • Vomiting in approx 1%( suggest repeat dose if vomit within 2 hrs LNG or 3 hours UPA) Repeat dose/offer IUD • Next menses; on average 1.2 days earlier with LNG, 2 days later with UPA
When to do pregnancy test? • If no period, pregnancy test should be positive 3 weeks after event of upsi.
Case three • 16 year old Mary has a chaotic cycle. She had sex with her new boyfriend last night and he did not have a condom. On further questioning she took LNG 3 weeks ago after having sex with someone else and has not had a period since. • What should you consider and how would you proceed?
Can the method be used again in the same cycle? • IUD can be used for multiple events in same cycle if fitted within 5 days earliest calculated date of ovulation • LNG can be used more than once in same cycle; even if the earlier episode of upsi was outside the treatment window( outside product licence)
Can the method be used more than once in same cycle? • UPA can not be used more than once in same cycle and cannot be used if LNG has been given earlier in the cycle. • UPA cannot be used if there has been an earlier UPSI event earlier in the cycle outside the treatment window of 120 hours.
Case four • Lorraine is 16. You saw her a week ago and provided LNG for her for upsi the night before. It is now 13 days since her last period which occur every 4 weeks. She admits when you ask that she also had sex 4 days ago but was afraid to mention it. Again she had not used a condom. • What is her EC method of choice?
Case four • Copper IUD deals with both episodes and is her best choice. • LNG can be used but is only 50% effective. • You have until day 19 in a 28 day cycle to fit IUD; ie you have 6 days to organise this. • If you arrange for her to have IUD fitted in 2 days time what else would you do?
What methods can be used together? • LNG>1 per cycle • LNG and IUD( recommended if considering IUD) • UPA and IUD • But not; LNG and UPA in same cycle • Or…….UPA>1 per cycle
Drug interactions with EC • LNG; reduced efficacy with liver enzyme inducers and for 28 days after. Offer copper IUD or if this is unacceptable a single 3mg dose LNG( outside product licence) • Eg St John’s Wort; use double dose • Concomitant use cyclosporin; increases toxicity; IUD preferred
Drug interactions with EC • UPA ; cannot be used if on liver enzyme inducers or for 28 days after this. • UPA; requires acidic pH in stomach; cannot be used if on antacids, PPI, H2 blocker • Also ;avoid UPA if severe asthma uncontrolled with oral steroids.
Investigations? • STI testing including HIV • Retest after appropriate window; 2 weeks for chlamydia • Consider prophylactic antibiotics with emergency IUD; stat dose azithromycin to cover chlamydia.
Future contraception • Oral EC does not provide contraceptive cover for further UPSi in same cycle. • Consider “quick start”;cocp, pop or implant with extra precautions. • IUD; can leave for future contraception/ remove when pregnancy excluded. If removing ensure adequate method/no sex for 7 days before removal.
Continuing current method • After LNG; condoms for 7d on cocp • for 2 days if on pop • for 9 days if on Qlaira • After UPA; condoms for 14 days on cocp • for 9 days if on pop • for 16 days Qlaira
What method should be offered? • Copper IUD should be offered to ALL WOMEN and DOCUMENT this. • Use of LNG > 72 hours would be unlicensed but supported by Clinical Effectiveness Unit for up to 96 hours • UPA is the only oral method licensed for 72 to 120 hours and is the preferred method if elligible.
Cost effectiveness? • Ulipristal is a cost effective alternative to levornogestrel for all women requesting EC. • Provision of EC however has not been shown to reduce the rate of unintended pregnancy or abortions.
Information required; summary • Medical eligibility • Efficacy of method • LMP and cycle length • Number episodes UPSI in cycle and when • Previous use EC in same cycle • Drug interactions • Need for additional precautions/ ongoing contraception
QOF target • Document “larc advice given” at the time of provision of oral EC ( or within next month)