Download
1 / 27
290 likes | 700 Views
Stress, Burnout and Psychosocial Support for Staff of the Emergency Medical Services. Jana Seblova (1), Dana Hlavackova (1), Vladimír Kebza (2), Jana Vignerova (2), Blanka Cepicka (3) Ministry of Health, EMS of the Central Bohemian Region (1) National Institute of Public Health (2)

E N D
Stress, Burnout and Psychosocial Support for Staff of the Emergency Medical Services Jana Seblova(1), Dana Hlavackova (1), Vladimír Kebza (2), Jana Vignerova (2), Blanka Cepicka (3) Ministry of Health, EMS of the Central Bohemian Region (1) National Institute of Public Health (2) S.E.N.A. Prague (3)
STUDY : „Stress of EMS professionals with special attention to burnout syndrome“ • 2003 – 2004 • Objectives: • to analyze sources of stress associated with profession • degree of exposition to critical incidents • to analyze postitive factors • study average and individual rates of burnout syndrome (BOS) • 2004 – 2006 • implementation of preventive and intervention psychological methods in the practice of EMS • 2005 - 2006 • evaluation of these interventions and rates of BOS
Questionnaires 2003/2005(created for the purpose of this study) • demographic items (age, sex, matrimonial status, position at work, lenght of practice, former specialization, postgraduate education…) • stressors and positive factors of the work in EMS – open questions + quantification (0-9), techniques of deescalation of stress (positive and negative) • exposition to critical incidents (predefined 5 indicators: death/injury on duty, multiple victim accidents, burn trauma, unsuccesful CPR or death of a child, endangering during duty – respondents were asked to specify) • screening questionnaire for burnout – 10 questions, simple rating (the same one used in the second phase)
Results: stressors in EMS practice • at least one stressor was named by 236 of 286 respondents (82,5%) • the most frequently named and the most intensive stressor was unsuccessful CPR or death of a child/young patient: 89 (31,1% of all respondents, average intensity 7,7 – maximum 9) • multiple victim accidents, disasters: 42 (14,7% - 6,5) • overtime hours, work in shifts, irregular life style: 38 (13,3% - 6,7) • interepesonal relations at work: 38 (13,3% - 5,9) • behaviour of the patients and relatives to EMS professionals: 35 (12,2% - 5,0) • work at medical dispatch – 28 of 51 dispatchers (54,9%)
Results: positive aspects of profession • helping other people and saving their health/lives (136 = 46,9%, intensity 7,4) • „action“ type of work, wchich in not boring (89 = 30,7%, intensity 6,8) • contacting people – as colleagues, and also as patients (80 = 27,6%, intensity 6,7) • flexibile spare time due to working in shifts (38 = 13,3%) – the same number of respondents see shifts and irregular life style as a stressor! • ambivalence: shifts, colleagues, salary…
Results: endangering during duty • 235 field professionals (included: physicians, emergency medical nurses, paramedics/EMTs, excluded: dispatchers) • 201 respondents (85,5%) experienced some form of endangering themselves during duty • ambulance car accident: 96 persons (40,1%), 21 physicians (48,8%), 18 EMTs (44%), 52 emergency medical nurses or paramedics (34,4%) • aggression (patient, relatives, friends…): 154 (65,5%), physicians 32 (74,4%), EMTs 28 (68,3%), emergency medical nurses and paramedics 83 (55%) – often named alcohol and drugs associated with aggression towards helath care professionals
Material and methods - burnout • 2003: 350 questionnaires sent, 290 returned (82,9%), 4 excluded (work position not defined) – 286 respondents • 2005: 750 questionnaires sent, 644 returned (85,8%), 597 respondents met inclusion criteria • (practice in EMS more than 1 year, half to full time job, agreement with participation) • basic comparison 2003/2005 and in 2005 group A = 372 (one or more psychological intervention) and B = 225 (no interventions) – using analysis of variance (ANOVA) • test of individual factor´s influence on BOS symptoms: General Linear Model (GLM), software SPSS, version 12 • the same comparison for each of four professional groups
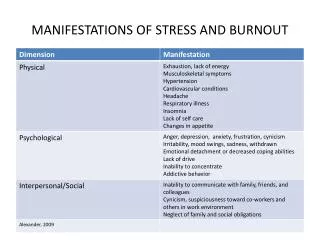
Results: symptoms of burnout • no significant difference 2003/2005 and in the year 2005 in the group with and without psychological interventions • in medical nurses statistical significant improvement between 2003/2005 (0,030) • highly significant difference between the group of dispatchers compared to any other professional group • the other factor influencing highly significantly symptoms of BOS is the length of practice in EMS • no other factor has influence on the degree of BOS (sex, matrimonial status, any professional position other than dispatcher, age…)
Results: symptoms of burnout • Variable Statistical significance (p) • ______________________________________________ • Sex 0,842 n.s. • Age 0,164 n.s. • Lenght of practice 0,002 • Matrimonial status 0,995 n.s. • Profesional position 0,000 • Group of respondents 0,697 n.s. • (2003 / 2005) • Intervention yes/no 0,771 n.s.
Preventive and intervention methods(2004 – 2006) • preventive and educational lectures • communication training (dispatchers, teams) • psychological consultations concerning professional stress and coping with it • structured interviews • CISM (Critical Incident Stress Management) after critical incidents (Mitchell´s model) • physicians, medical nurses, paramedics, dispatchers
Satisfaction with psychological interventions • preventive and educational lectures …………………92% • communication training…………………………………92% • CISM (Critical Incident Stress Management) • after critical incidents………………………………….. 83% • structured interviews………………………………….…81% • psychological consultations concerning • professional stress and coping with it…………………79%
Conclusions of the study: • the only 2 factors influencing highly significantly symptoms of BOS are the position of dispatcher and length of practice in EMS • psychological techniques can improve the level of well-being of professionals, possible influence in the future - all kinds of interventions were postitively accepted • specific programmes are used for dispatchers as the amount of their professional stress is significantly higher and these programmes should be recommended for wider application • concentration on safe driving the ambulance car as prevention of accidents • specific intervention programme for victims of aggression should be created
Implementation of psychological techniques • Education, preventive lectures: • EMS professionals – CME certified • middle management • dispatchers – CME certified • Communication training: • emergency nurses, paramedics, physicians • dispatchers • Supervision • field teams, dispatchers – feedback for management • individual supervision – on demand • top management • Consultations concerning professional stress • co-operating psychologist, based on obligatory professional secret
Building the system of CISM • CISM – a system of preventive and intervention techniques • certified CISM courses – Dr. Thomas Appel-Schumacher, University of Maryland – 2004 (2 participants), 2006 and 2007 (organized by Ministry of Health, 15 + 10 participants) – some of them joined the system on voluntary basis as peers • crisis intervention: obligatory after large scale disasters • implemented in „Protocol for Major Incident“ • in contract between organization and trade unions (care of employees) • Medical Director – the role of CISM coordinator (indication, type and timing of intervention, contacting mental health professional, logistics)
CISM in practice of EMS of the Central Bohemian region • the first debriefing: after activation of disaster plan after serious traffic accident of a bus 6. 7. 2006, high mortality of victims, debriefing after 10 days from the accident • 3. 11. 2006: a traffic accidents of 2 ambulances and 1 police car in one emergency call (South Bohemian EMS) – a serious injury of emergency nurse and the rest of teams were also injured • 28. 7. 2007:activation of disaster plan - the thieves of iron caused a serious destruction of a former factory´s hall, some of the people were of entrapped, unknown number of affected people, danger for the rescuers….
CISM in practice of EMS of the Central Bohemian region • 12. 4. 2008 – the emergency teams sent to the highway traffic accident, another car had crashed into the ambulance on scene, one dead victim and all injured members of the EMS team; they were trying to help all the other victims despite their own injuries untill other ambulances came on scene • 20. 10. 2008 – a car crash of ambulance with physician, the screw of the other ambulance provided first aid to the victims = colleagues • 15. 5. 2009 – the drunken patient attacked the screw (2 males, 1 female – all injured)
Pilot project of Ministry of Health and EMS of the Capital Prague • study on stress nad burnout of all medical personnel including dispatchers compared to non-medical personnel • Maslach Burnout Inventory • high scores in emotional exhaustion • system of providing support based on group of peers (10 peers) with mental health professional´s supervision • voluntary basis with reimbursement in case of providing intervention • need for psychosocial support proved – average number of contacts 15/month • possible model for national system
National System of crisis intervention • since 2009, organised by Ministry of Health – Department of Crisis Preparedness • working group for building national system of crisis intervention • a part of Departments of crisis management in organisations • Providers: • EMS (regional system of emergency care – 14 organisations) – in the next period co-operation with Police anf firefighters is planned (within „Integrated Rescue System“) • hospitals – University teching hospitals, regional… • regional authorities • volunteers and NGO´s
National System of crisis intervention • Primary goals: • terminology, definition of tasks and responsibilities • database of peers • coordination on regional level • system of communication in case of need of intervention (individual vs. major incident) – telephone line 24/7/365 • education of providers • financial resources • evaluation and feedback • PR