Download
1 / 63

E N D
Introduction • Landmarks: abdomen is a large oval cavity extending from the diaphragm down to pelvic brim. in back bordered by vertebral column muscles, at the sides & front by the lower rib cage & abdominal muscles, 4 layers of muscles joined at midline called linea alba, one the rectus abdomenis edge is palpable.
- Anatomy: • all internal organs are the viscera, solid viscera are those that maintain a characteristic shape (liver, pancreas, spleen, kidneys..). the shape of hollow viscera • ( stomach, gallbladder, colon & bladder) depends on the contents. Usually are not palpable.
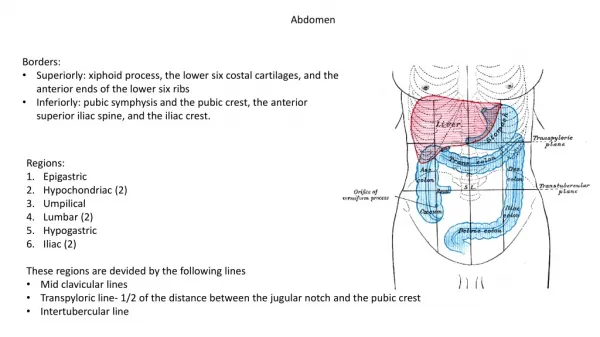
abdominal wall is divided into 4 quadrants by a vertical & horizontal line bisecting umbilicus(old system divided abdomen to 9 regions). • Page 565+ slide
1- Appetite, weight change 2- Dysphagia 3- Food intolerance 4- Abdominal pain onset, duration, severity, location, radiation, associated factors, quality, ↑-↓ factors) 5- Nausea/ vomiting 6- Bowel habits 7- Past abdominal history 8- Medications 9- Nutritional assessment ** Subjective Data:
** Objective Data: · Preparation: - Expose abdomen • enhance abdominal relaxation • empty bladder • warm room, warm stethoscope endpieces & your hands • person supine, head on pillow, arms at sides • short fingernails • examine painful areas at last • use distraction through breathing exercises, low voice.
** ISPECT THE ABDOMEN: • Contour: stand on the Rt side look down to abdomen, then sit to gaze across abdomen,, determine the profile from rib margin to pubic bone. Ranges from flat to rounded (flat-scaphoid-rounded- protuberant). • Symmetry: shine a light across abdomen, should be symmetrically bilateral. note any bulging, visible mass or a symmetric shape, ask person to take deep breath or ask him to sit up without pushing up with his hands.
Umbilicus: midline & inverted, no sign of discoloration, inflammation, or hernia. • Skin: smooth& even, homogeneous color. common pigment change is straie, silvery white linear marks about 1-6 cm long, recent straie are pink or blue, then they turn silvery white. Moles, circumscribed brown macular or popular areas, are common on the abdomen, no lesions, if scar present draw its location in his record, indicating length in cm (possible underlying adhesions &excess fibrous tissue). Skin turgor (gently pinch up a fold of skin then release)
Pulsation or movement: normally see pulsations from aorta in epigastric area, respiratory movement in abdomen in males, waves of peristalsis sometimes are visible in very thin persons. • Hair distribution: pubic hair growth normally has a diamond shape in adult males & an inverted triangle shape in adult females • Demeanor: a comfortable person is relaxed, benign facial expression & slow even respiration.
** AUSCULTATE BOWEL & VASCULAR SOUNDS: • its done before palpation & percussion because they can increase peristalsis which would give a false interpretation of bowel sounds. use diaphragm endpiece because bowel sounds are high pitched, hold lightly against skin. Begin in RLQ because bowel sounds are always present here normally.
Bowel sounds: • note character & frequency; originate from the movement of air & fluid through small intestine (5-30 times/min). Don’t bother to count them, judge if normal, hypoactive, or hyperactive. One type of hyperactive bowel is hyperperistalsis when you feel your “stomach growling” termed boborygmus, you must listen for 5 min before deciding absent bowel sounds.
Vascular Sounds: • note the presence of any vascular sounds or bruits using firmer pressure, over aorta, renal arteries, iliac, & femoral, usually no such sound is present.
** PERCUSS TYMPANY, LIVER SPAN, & SPLENIC DULLNESS: • assess the relative density of abdominal content, to locate organs & to screen for abnormal fluid or masses.
General tympany : • percuss in all 4 quadrants, tympany should predominate because air in the intestine rises to the surface when the person is supine.(dullness over distended bladder- hyperresonanace with gaseous distention).
Liver span: • percuss to map out the boundaries of certain organs. Measure the height of liver in Rt MCL, begin in the area of lung resonance & percuss down the interspaces until the sound changes to a dull quality. mark the spot, usually 5th ICS, then find abdominal tympany & percuss up in MCL, mark where the sound changes from tympany to a dull sound, normally at the Rt costal margin. measure the distance between the 2 marks ,
normal liver span in adult 6-12 cm , taller people have longer livers, males have a larger liver span than females of same height, mean liver span is 10.5 cm for males& 7 cm for females. (Enlarged liver span indicate hepatomegaly). • in emphysema liver displaced downward by hyperinflated lungs, but liver span still within normal. in ascitis or gas distention its pushed up .
# Scratch Test: • help define liver border when abdomen is distended or abdomen muscles are tense, place your stethoscope over liver, with one fingernail, scratch short strokes over abdomen, starting in RLQ & moving up , when the scratching sound becomes magnified, you have crossed the border from over a hollow organ to a solid one.
Splenic Dullness: • · a dull note from 9th to 11th ICS just behind the Lt MAL, not wider than 7 cm, now percuss in lowest interspace in Lt AAL, tympany should result, tympany remain through full inspiration.
Costovertebral Angle Tenderness: • indirect fist percussion causes tissues to vibrate instead of producing a sound. To assess kidney, place one hand over 12th rib at costovertebral angle on back. Thump with ulnal edge of your other fist, normally person feels a thud but no pain (done while examine thorax)
Special procedures: • if suspect person has ascitis (free fluid in the peritoneal cavity) because of distended abdomen, bulging flanks, protruded umbilicus, you can differentiate ascitis from gaseous distention by performing 2 percussion tests.
# Fluid wave: • test for fluid wave by standing on Rt side, place ulnar edge of another examiner’s hand or patient hand firmly on abdomen in midline (this stop transmission across skin of upcoming tap). Place your Lt hand on the person’s right flank. With your Rt hand give Lt flank a firm strike. If ascitis is present, the blow will generate a fluid wave through the abdomen & you will feel a distinct tap on your Lt hand. If the abdomen is distended from gas or adipose tissue you will feel no change.
# Shifting Dullness: • in supine position, ascitic fluid settles by gravity into flanks, displacing air-filled bowel upward, percuss down the side of abdomen. If fluid is present the note will change from tympany to dull as you reach its level. Mark this spot. Now turn him onto Rt side (roll him toward you), fluid will gravitate to dependent (Rt) side,
displacing lighter bowel upward. Begin percussing upper side of abdomen & move downward. Sound changes from tympany to a dull sound as you reach fluid level; dullness is higher, upward toward umbilicus. Shifting dullness is positive with a large volume of ascitic fluid, detect if more than 500 ml of fluid. Both tests are not reliable; U/S study is a definite tool.
PALPATE SURFACE & DEEP AREAS: • perform palpation to judge the size, location& consistency of certain organs, & to screen for abnormal mass or tenderness, use additional measures to enhance complete muscle relaxation: • 1- bend person’s knee • 2- keep your hand low & parallel to abdomen • 3- breath slowly • 4- keep your own voice low &soft • 5- Imagery • 6- ticklish person Use his own hands under yours. • 7- Perform palpation just after auscultation
** Light & Deep palpation: • Begin with light palpation, first 4 fingers close together depress the skin about 1 cm, make a gentle rotary motion, then lift the fingers (don’t drag them)& move clockwise, around the abdomen to form overall impression of skin surface & superficial musculature, any identified tender areas until last. Discriminate between voluntary muscle guarding & involuntary rigidity, voluntary guarding occurs when the person is cold, tense, or ticklish, its bilateral, muscles relaxed slightly during exhalation, if rigidity persists its involuntary.
Now perform deep palpation, but push down about 5-8 cm, moving clockwise, to overcome the resistance of a very large or obese abdomen, use a bimanual technique, place two hands on top of each other, the top hand does the pushing, the bottom hand sense of palpation, note the location, size, consistency & mobility of palpable organs, tenderness, or masses.
- mild tenderness normally is present when palpating sigmoid colon, other tenderness should be investigated. • - if you identify a mass, first distinguish it from a normally palpable structure or an enlarged organ. Then note the following:
1- location 2- size 3- shape 4- consistency(soft, firm, hard) 5- surface(smooth, nodular) 6- mobility 7- pulsatility 8- tenderness
** LIVER: • Begin palpation with liver in RUQ, place your Lt hand under the person’s back parallel to 11th & 12th ribs & lift up to support the abdominal contents, place your Rt hand on RUQ with fingers parallel to midline. Push deeply down & under the Rt costal margin. Ask the person to take a deep breath, its normal to feel the edge of the liver bump your fingertips during inhalation, feels like a firm regular ridge, liver often not palpable & you feel nothing firm.
# Hocking technique: • stand up at person’s shoulder & swivel your body to Rt so that you face the person’s feet. Hook your fingers over costal margin from above. ask person to take a deep breath, feel the liver edge bump your fingertips.
# SPLEEN: • Normally its not palpable & must be enlarged 3 times its size to be felt. Reach Lt hand over abdomen & behind Lt side at the 11th &12th ribs. lift up for support. Place your Rt hand obliquely on LUQ with fingers pointing toward the Lt axilla & just inferior to rib margin. Push your hands deeply down & under Lt costal margin & ask person to take a deep breath, you should feel nothing firm.