Download
1 / 62
630 likes | 774 Views
Abdomen. Adapted from Mosby’s Guide to Physical Examination, 6 th Ed. Ch. 17. Tips…. Perform early in the exam Relaxation and quiet Bottle/pacifier/nursing On parent’s lap Dr. sits facing the parent, knees touching. Ticklish?. Firm touch Place the child’s hand under your palm

E N D
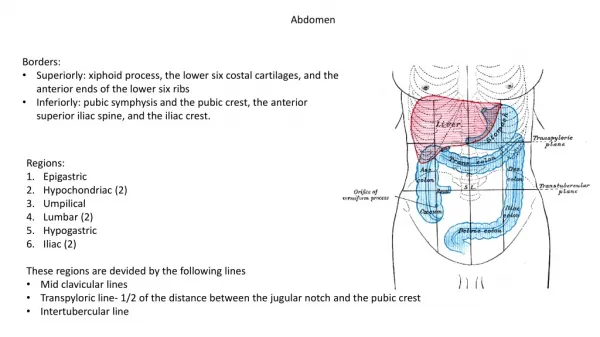
Abdomen Adapted from Mosby’s Guide to Physical Examination, 6th Ed. Ch. 17
Tips… • Perform early in the exam • Relaxation and quiet • Bottle/pacifier/nursing • On parent’s lap • Dr. sits facing the parent, knees touching
Ticklish? • Firm touch • Place the child’s hand under your palm • leaving your fingers free to palpate
Tenderness and pain can be difficult to detect/assess Look for: • Change in pitch of crying • Facial grimace • Rejection of the opportunity to suck • Drawing the knees to the abdomen
Localizing Pain • Distract the child with a toy • Start away from the area suspected • Observe for changes… as you move to identify the area of greatest pain • facial expression • constriction of pupils
If a child will not stop crying… • Use the respiratory cycle • Abdomen should be soft during inspiration • If abdomen remains hard during both inspiration and expiration • Noticeable rigidity • Resistance to pressure …suspect peritoneal irritation
Inspection • Shape • Contour • Movement with respiration Note • localized fullness • scaphoid • protrusion (above the level of the chest)
Infant abdomen should be… • Rounded and dome shaped • musculature has not fully developed • Abdominal and chest movements should be synchronous • slight bulge of the abdomen at the beginning of respiration
Distended abdomen • Feces, mass, organ enlargement Scaphoid abdomen • Abdominal contents are displaced
Pulsations - epigastric area • Common in newborns and infants Distended veins across the abdomen • Vascular obstruction • Abdominal distension or obstruction Spider nevi • Liver diease
Newborn - Umbilical Cord Count the vessels • 2 arteries, 1 vein *Single umbilical artery… possible congenital anomolies
Umbilical Stump • Should be dry and odorless Inspect all skin folds for: • Discharge • Redness • Induration • Skin warmth • Granulomatous tissue
Umbilicus is usually inverted • Note any protrusion through the umbilicus or rectus abdominus muscle • Hernia • Diastasis recti *Often everts with increased abdominal pressure
Peristaltic Waves • Use tangential lighting • Observe abdomen at eye level • Usually not visible • Sometimes seen in thin, malnourished babies • Suggests intestinal obstruction • Pyloric stenosis • Frequent vomiting…
Auscultation • Peristalsis • “Metalic tinkling” • Heard every 10-30 seconds • Bowel sounds should be present 1-2 hours after birth • No bruits or venous hum should be detected
Renal Bruits • Patient held upright/sitting • Listen at the posterior flank • Supine • Listen over the abdomen Renal artery stenosis • High frequency, soft Renal arteriovenous fistula (rare) • Continuous
Palpation With infant’s feet slightly elevated, knees flexed… Superficial palpation • Identify the spleen, liver, and masses close to the surface
*Can seem tiny compared to the size of your hand… • Place your hand gently on the abdomen • Thumb at the right upper quadrant • Index finger at the left upper quadrant • Press very gently at first, only gradually increasing pressure • Palpate over the entire abdomen
Spleen • First few weeks, palpable 1-2 cm below the left costal margin • Detectable spleen tip (left costal margin) • common in well infants Increase in spleen size may indicate: • blood dyscrasias • septicemia
Liver Estimation of true liver size (liver span) • Percuss the upper border • Palpate the lower edge Upper edge • 5th intercostal space at the right midclavicular line
Lower edge • Palpate the right midclavicular line 3-4 cm below the costal margin • Gradually move your fingers up until you feel the mass come down as the infant inspires Newborn: • just below the right costal margin Infants & toddlers: • 1-3cm below the right costal margin Children: • 1-2cm below the right costal margin
Hepatomegaly Liver is >3 cm below the right costal margin Indicates possible: • Infection • Cardiac failure • Liver disease
Deep Palpation Palpate all quadrants for masses • Location • Size • Shape • Tenderness • Consistency *Transillumination • Distinguish cystic from solid masses
Fixed masses should be investigated with special studies if… • Laterally mobile • Pulsatile • Palpate the aorta for signs of enlargement • Located along vertebral column If any suspicion of neoplasm exists, limit palpation of the mass. May cause injury or spread of malignancy!
Percussion • May be more tympanic (vs. adults) • Swallow air when feeding & crying Tympany with distended abdomen? • Gas Dullness with distended abdomen? • Fluid, solid mass
Examine the bladder • Palpate and percuss • suprapubic area • Determine size • Distention?
Toddlers • Abdomen protrudes slightly “Potbellied” • Seated, standing or supine After age 5 • Abdomen (supine) may become convex when laying supine
Abdominal Respirations • Respirations continue to be abdominal until 6-7 years of age • If persists past the age of 7, may suggest a thoracic problem • In young children restricted abdominal respiration may be related to: • Peritoneal irritation • Acute abdomen
Rebound Tenderness • Observe child’s facial expression and pupils • Be cautious! Once a child has experienced palpation that is too intense, a subsequent examiner has little chance for easy access to the abdomen.
Granuloma • Serous or serosanguinous discharge once the stump has separated • No other signs of infection
Omphalocele • Intestine present in the umbilical cord or protruding from the umbilical area • Visible through a thick transparent membrane
Umbilical Hernia • Protrusion of omentum and intestine through the umbilical opening • Common in infants • Reach maximum size by1 month of age • Generally close spontaneously • 1-2 years of age • Reduces temporarily • push contents in (lightly) and it pops right out again
May be very large and impressive • Apparent size is not cause for alarm To determine size: • Measure the diameter of the opening, not the protruding contents
Diastasis Recti • Midline separation (rectus abdominus) • 1-4 cm wide • between xiphoid and umbilicus • No need to repair in most cases • Resolves by 6 years of age *Herniation through the rectus abdominus does require surgery
What if you find… ? • Sausage-shaped mass • Left lower quadrant • Feces in the sigmoid colon …Constipation • Midline, surpapubic mass • Feces in the rectosigmoid colon …Hirschsprung disease
Hirschsprung Disease (Congenital Aganglionic Megacolon) • Absence of parasympathetic ganglion cells in a segment of the colon • Absence of peristalsis • Feces accumulate proximal to the defect • Leads to intestinal obstruction
Signs & symptoms: • Failure to thrive • Constipation • Abdominal distention • Episodes of vomiting and diarrhea Newborn: • may fail to pass meconium in the first 24-48 hrs Older infants and young children: • intestinal obstruction or severe constipation
What if you find… ? • Sausage-shaped mass • Left or right upper quadrant …Intussusception
Intussusception • Prolapse of one segment of intestine into another • Causes intestinal obstruction • Cause is unknown • mc 3-12 months old
Signs & symptoms: • Acute intermittent abdominal pain • Abdominal distention • Vomiting • Stools mixed with blood and mucus • Red current jelly appearance • Sausage-shaped mass in R or L upper quadrant • R lower quadrant feels empty (Dance sign)
Dramatic onset • Apparently well child starts crying suddenly and excruciatingly • awaken from sleep • Doubling up with pain • Inconsolable Episode may cease abruptly but symptoms will most likely recur…
Intussusception – “ABCDEF” • Abdominal or anal “sausage” • Blood from the rectum • Colic: babies draw up their legs • Distention, dehydration, and shock • Emesis • Face pale
What if you find… ? • Olive-shaped mass (deep palpation) • Right upper quadrant • Immediately after the infant vomits …Pyloris stenosis
Pyloric Stenosis • Hypertrophy of the circular muscle of the pylorus • obstruction of the pyloric sphincter • 1st month after birth
Signs & symptoms: • Regurgitation ~> projectile vomiting • vigorous, shoots out of the mouth, carries a short distance • Feeding eagerly • even after vomiting • Failure to gain weight • Signs of dehydration • Small, rounded mass palpable in the R upper quadrant • especially after the child vomits
Gastroesophageal Reflux • Relaxation or incompetence of the lower esophagus persisting beyond the newborn period
Signs & symptoms: • Regurgitation and vomiting • weight loss and failure to thrive • Respiratory problems • aspiration • Bleeding from esophagitis