Download
1 / 118
1.21k likes | 1.46k Views
ABDOMEN. Hepatobiliary. Hepatobiliary :. Cavernous Hemangioma Choledochal Cysts Choledocholithiasis Fatty Infiltration of the Liver Focal Nodular Hyperplasia Homochromatosis Hepatic Adenoma Hapatic Cysts Hepatic Metastases Hepatoma. CAVERNOUS HEMANGIOMA. Description:.

E N D
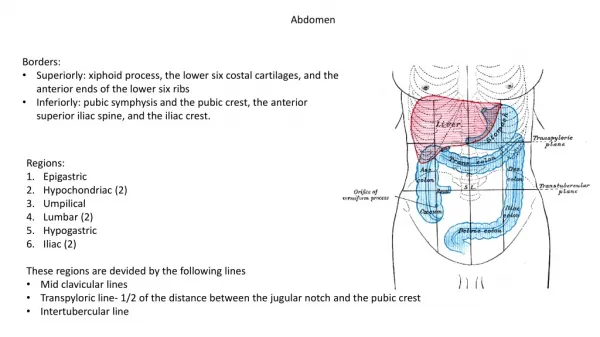
ABDOMEN Hepatobiliary
Hepatobiliary: • Cavernous Hemangioma • Choledochal Cysts • Choledocholithiasis • Fatty Infiltration of the Liver • Focal Nodular Hyperplasia • Homochromatosis • Hepatic Adenoma • Hapatic Cysts • Hepatic Metastases • Hepatoma
Description: • Cavernous hemangiomas are the most common benign hepatic tumors. Found as either single or multiple tumors. They are usually small, measuring 1 to 2 cm in diameter. These tumors are mostly silent with only a small percentage being symptomatic.
Etiology: • These vascular malformations are composed of large dilated endothelium lined vascular channels covered by a fibrous capsule.
Epidemiology: • Occur in all age groups. Are more common in females than males. The incidence rate is approximately 1% to 2% in the normal adult population and up to 20% at autopsy.
Signs and Symptoms: • Usually in an incidental finding on large symptomatic tumors, upper abdominal pain is experienced.
Imaging Characteristics: CT • Noncontrast studies appear hypodense. • Early peripheral contrast enhancement whereas the central portion of the lesion remains low density. Sequential scan over a period of time demonstrates progressive contrast filling of the lesion central low density progressively becoming smaller.
MRI • T1-weighted images appear hypointense. • T2-weighted images appear hyperintense. • T1-weighted contrast-enhanced images appear hyperintense with increasing signal over 15 to 30 minutes following injection.
Treatment: • Surgical intervention is usually not required unless the tumor is large and symptomatic.
Prognosis: • Good; these are benign tumors.
Figure 1. Cavernous Hemangioma T1-weighted MRI of the liver shows round low-signal-intensity mass (arrow) in the posterior segment of the right lobe of the liver.
Figure 2. Cavernous Hemangioma T2-weighted MRI of the liver shows this lesion to be very bright (high signal intensity).
Figure 3. Cavernous Hemangioma Early postcontrast gradient-echo MRI of the liver shows peripheral enhancement of the mass lesion.
Figure 4. Cavernous Hemangioma Delayed postcontrast gradient-echo MRI of the liver shows contrast filling of this lesion.
Description: • A choledochal cyst is a focal dilatation of the bile duct.
Etiology: • Choledochal cysts are considered to be a congenital anomaly of the biliary tree.
Epidemiology: • More commonly seen in females than males. Patients may be clinically symptomatic before 10 years of age.
Signs and Symptoms: • Though not seen in all patients, the classic clinical triad of symptoms include pain, jaundice, and a palpable abdominal mass in the upper right quadrant.
Imaging Characteristics: • A cystic dilatation of the extrahepatic bile, with or without dilatation, of the intrahepatic bile duct. CT • Demonstrates a cystic mass in the portahepatis that appears with an approximate density of water.
MRI • Low signal from within the cyst is seen on T1-weighted images. • High signal from within the cyst is seen on T2-weighted images. • MR cholangiopancreatography (MRCP) is the best noninvasive test for the diagnosis of choledochal cyst. • MRCP shows localized dilation of the common bile duct.
Treatment: • Surgical resection is often performed because of the risk of malignancy associated with this disorder.
Prognosis: • If the obstruction is not corrected, infections and chronic liver disease can develop. In the case of a cancerous tumor, complete resection and therapy produce a 5-year survival rate of 30% to 40%.
Figure 1. Choledochal Cyst MRCP in the coronal plane shows a fusiform dilatation of the common bile duct. This is consistent with a Type I choledochal cyst.
Figure 2. Coronal MIP MRCP in a different patient showing a Type IV choledochal cyst.
Figure 3. CECT axial (A) and coronal MPR (B) images show a Type IV choledochocyst.
Description: • Choledocholithiasis is a calculi or stone in the common bile duct. These calculi usually form in the gallbladder and move into the common bile duct.
Etiology: • Stones consisting primarily of cholesterol develop in the gallbladder and enter into the common bile duct.
Epidemiology: • Approximately 10% to 50% of patients with cholecystitis have stones in the common bile duct. The incidence rate increase with age and is seen more frequently in females.
Signs and Symptoms: • The patient is asymptomatic when there is no obstruction. Abdominal pain in the epigastric region, nausea indicates an obstruction of the common bile duct. Other signs could include pancreatitis and a palpable gallbladder.
Imaging Characteristics: CT • Stones with a high attenuation (hyperdense) may be seen without IV contrast. • MRI • MR cholangiopancreatography (MRCP) is the best noninvasive study for the diagnoses. • MRCP demonstrates the stone as hpointense defect in the common bile duct (CBD).
Treatment: • Endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy and stone removal in most cases. Surgical removal is rarely needed.
Prognosis: • Good with early diagnosis and treatment. The patient may experience complications secondary to obstruction of the CBD such as jaundice, cholangitis, and pancreatitis.
Figure 1. Choledocholithiasis ERCP shows a dilated common bile duct with a distal filling defect (arrow) consistent with choledocholithiasis.
Figure 2. Choledocholithiasis Axial CECT shows a radiodense stone (arrow) in the dilated distal common bile duct.
Figure 3. Choledocholithiasis MRCP shows multiple hypointense stones in the gallbladder (short arrow) as well as a similar-appearing stone in the dilated distal common bile duct (long arrow).
Figure 4. Choledocholithiasis Coronal MRCP shows the hypointense stone within the dilated common bile duct (arrow).
Description: • Fatty infiltration of the liver is the result of excessive depositions of triglycerides and other fats in the liver cells.
Etiology: • This condition appears in association with a variety of disorders such as obesity, malnutrition, chemotherapy, alcohol abuse, steroid use, parenteral nutrition Cushing syndrome, and radiation hepatitis. In the United States, the most common cause is related to alcoholism.
Epidemiology: • In the United States, this disorder is commonly associated with the overuse of alcohol.
Signs and Symptoms: • Fatty liver is usually “silent” but may be associated with hepatomegaly and abdominal pain in the right upper quadrant.
Imaging Characteristics: • CT is the modality of choice for diagnosing fatty infiltration of the liver. CT • Fatty infiltration may be focal or diffusely distributed within the liver. • Fatty infiltrates demonstrate a lower (hypodense) attenuation in appearance in comparison to the spleen on noncontrast studies. • MRI • T1- and T2-weighted images may demonstrate an increase in signal when compared to normal liver parenchyma. • The STIR sequence suppresses the signal from fat when compared to above pulse sequences.
Treatment: • Supportive and consists of correcting the underlying condition or eliminating its cause (eg, alcohol) and focusing on proper nutrition.
Prognosis: • Depends on the underlying condition or etiology.
Figure 1. Fatty Infiltration of the Liver CT of the abdomen with IV contrast shows mildly enlarged liver. There is diffuse low attenuation of the liver compared to the spleen consistent with fatty infiltration. Note: The contrast opacified hepatic and portal veins against the low-density back-ground of the liver appear bright.
Description: • Focal nodular hyperplasia (FNH) is a benign, tumor-like lesion.