Download
1 / 37
370 likes | 374 Views
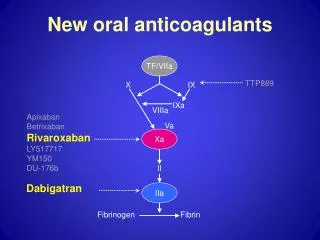
UPDATE ON DIRECT ORAL ANTICOAGULANTS: A PERSPECTIVE BEYOND THE CANCER-VTE GUIDELINES. Cristhiam M. Rojas-Hernandez, MD Assistant Professor Section of Benign Hematology. Faculty Disclosure. UPDATE ON DIRECT ORAL ANTIACOAGULANTS. OBJECTIVES.

E N D
UPDATE ON DIRECT ORAL ANTICOAGULANTS:A PERSPECTIVE BEYOND THE CANCER-VTE GUIDELINES Cristhiam M. Rojas-Hernandez, MD Assistant Professor Section of Benign Hematology
UPDATE ON DIRECT ORAL ANTIACOAGULANTS OBJECTIVES • To review the cancer subgroup-clinical trial data for the management of VTE. • To review the efficacy and safety outcomes of exploratory cohort data in cancer related-VTE. • To review the available data on the selection and use of anticoagulants in clinical practice outside clinical trials. • To summarize practical clinical considerations for the use of direct oral anticoagulants in the cancer population.
ARE THE DIRECT ANTICOAGULANTS SAFE AND EFFECTIVE IN CANCER-VTE?
CANCER SUBGROUP-CLINICAL TRIAL DATA VTE Agnelli, et al (2015). Journal of thrombosis and haemostasis : JTH 13 (12):2187-2191. Prins, et al (2014). The Lancet Haematology 1 (1):e37-46. Raskob, et al (2016). The Lancet Haematology 3 (8):e379-387. Schulman, et al (2015). Thrombosis and haemostasis 114 (1):150-157.
CANCER SUBGROUP-CLINICAL TRIAL DATA VTE EFFICACY OUTCOME SYMPTOMATIC RECURRENT VENOS THROMBOEMBOLISM
CANCER SUBGROUP-CLINICAL TRIAL DATA: RECURRENT VENOUS THROMBOEMBOLISM OUTCOMES POPULATION WITH CANCER DIAGNOSIS AT STUDY ENROLMENT Agnelli, et al (2015). Journal of thrombosis and haemostasis : JTH 13 (12):2187-2191. Prins, et al (2014). The Lancet Haematology 1 (1):e37-46. Raskob, et al (2016). The Lancet Haematology 3 (8):e379-387. Schulman, et al (2015). Thrombosis and haemostasis 114 (1):150-157.
CANCER SUBGROUP-CLINICAL TRIAL DATA: RECURRENT VENOUS THROMBOEMBOLISM OUTCOMES POPULATION WITH CANCER DIAGNOSIS DURING STUDY FOLLOW-UP Prins, et al (2014). The Lancet Haematology 1 (1):e37-46. Raskob, et al (2016). The Lancet Haematology 3 (8):e379-387. Schulman, et al (2015). Thrombosis and haemostasis 114 (1):150-157.
CANCER SUBGROUP-CLINICAL TRIAL DATA VTE SAFETY OUTCOME CLINICAL RELEVANT BLEEDING
CANCER SUBGROUP-CLINICAL TRIAL DATA VTE DEFINITION OF MAJOR BLEEDING • Fatal bleeding, and/or • Symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intra-articular or pericardial, or intramuscular with compartment syndrome, and/or • Bleeding causing a fall in hemoglobin level of 20 g L−1or more, or leading to transfusion of two or more units of whole blood or red cells. Schulman, et al (2005). Journal of Thrombosis and Haemostasis, 3: 692–694.
CANCER SUBGROUP-CLINICAL TRIAL DATA: CLINICAL RELEVANT BLEEDING OUTCOMES POPULATION WITH CANCER DIAGNOSIS AT STUDY ENROLMENT Agnelli, et al (2015). Journal of thrombosis and haemostasis : JTH 13 (12):2187-2191. Prins, et al (2014). The Lancet Haematology 1 (1):e37-46. Raskob, et al (2016). The Lancet Haematology 3 (8):e379-387. Schulman, et al (2015). Thrombosis and haemostasis 114 (1):150-157.
CANCER SUBGROUP-CLINICAL TRIAL DATA: CLINICAL RELEVANT BLEEDING OUTCOMES POPULATION WITH CANCER DIAGNOSIS DURING STUDY FOLLOW-UP Prins, et al (2014). The Lancet Haematology 1 (1):e37-46. Schulman, et al (2015). Thrombosis and haemostasis 114 (1):150-157.
CANCER SUBGROUP-CLINICAL TRIAL DATA: MAJOR BLEEDING OUTCOMES POPULATION WITH CANCER DIAGNOSIS AT STUDY ENROLMENT Agnelli, et al (2015). Journal of thrombosis and haemostasis : JTH 13 (12):2187-2191. Prins, et al (2014). The Lancet Haematology 1 (1):e37-46. Raskob, et al (2016). The Lancet Haematology 3 (8):e379-387. Schulman, et al (2015). Thrombosis and haemostasis 114 (1):150-157.
CANCER SUBGROUP-CLINICAL TRIAL DATA: MAJOR BLEEDING OUTCOMES POPULATION WITH CANCER DIAGNOSIS DURING STUDY FOLLOW-UP Prins, et al (2014). The Lancet Haematology 1 (1):e37-46. Schulman, et al (2015). Thrombosis and haemostasis 114 (1):150-157.
NON-RANDOMIZED STUDY COHORT DATA Bott-Kitslaar, et al (2016). The American journal of medicine 129 (6):615-619. Mantha, et al (2017). Journal of thrombosis and thrombolysis 43 (2):166-171. Ross JA, et al (2017). Thrombosis research 150:86-89. Pignataro, et al. (2016) Clinical and applied thrombosis/Hemostasis.
WHICH ARE THE ANTICOAGULANTS PRESCRIBED FOR CANCER-VTE OUTSIDE CLINICAL TRIALS?
GUIDELINE STATEMENTS FOR CANCER-VTE “Use of novel oral anticoagulants for either prevention or treatment of VTE in patients with cancer is not recommended at this time.” “In the absence of cancer-specific studies, newer oral anticoagulants cannot be currently recommended.” “In patients with DVT of the leg or PE and cancer, as long-term (first 3 months) anticoagulant therapy, we suggest LMWH over VKA therapy, dabigatran, rivaroxaban, apixaban, or edoxaban.” “Direct oral anticoagulants can be considered for VTE treatment of patients with stable cancer not receiving systemic anticancer therapy, and in cases where VKA is an acceptable, but not an available, treatment choice.” “After 3–6 months, termination or continuation of anticoagulation (LMWH, VKA, or direct oral anticoagulants) should be based on individual assessment of the benefit-to-risk ratio, tolerability, drug availability, patient preference, and cancer activity.” Lyman, et al (2015). J Clin Oncol 33 (6):654-656. Di Nisio, et al (2015). Journal of Thrombosis and Haemostasis 13 (5):880-883. Farge, et al (2016). The Lancet Oncology 17 (10):e452-e466. Kearon, et al. (2016) Chest. 2016;149(2):315-352.
U.S. PRESCRIPTION PATTERNS FOR CANCER-VTE n = 105,399 Khorana, et al (2016). Thrombosis research 145:51-53.
U.S. PRESCRIPTION PATTERNS FOR CANCER-VTE Khorana, et al (2016). Thrombosis research 145:51-53.
U.S. PRESCRIPTION PATTERNS FOR CANCER-VTE Khorana, et al (2016). Thrombosis research 145:51-53.
CANCER-VTE: THE PATIENT EXPERIENCE • Semi-structured interviews with patients with cancer-associated VTE. • Data collected on 40 patients: • Treatments for cancer • Understanding and acceptability of LMWH • Positive and negative aspects of LMWH • Most of the patients had been on warfarin before. Noble, et al (2005). Palliative medicine 19 (3):197-201
CANCER-VTE: THE PATIENT EXPERIENCE • Acceptability of LMWH “The heparin is more than acceptable. . . . so much of my treatment has been sitting back and having things done to you . . . I prefer this . . . I feel that I have got control back in my life.” “It’s no problem, a little sting and then its over” Noble, et al (2005). Palliative medicine 19 (3):197-201
CANCER-VTE: THE PATIENT EXPERIENCE • Simplicity of LMWH (when compared to warfarin) “Every day my blood was checked and every day the dose of warfarin was changed . . . Eventually they started me on heparin . . . I wish they’d done it sooner . . . a quick injection and then you’re done . . . no blood tests no hassle” Noble, et al (2005). Palliative medicine 19 (3):197-201
CANCER-VTE: THE PATIENT EXPERIENCE • Optimism “I can’t beat the tumor but I can fight its effects . . . the heparin helps me face the future. I choose to inject myself because I feel I can face the future on my own terms . . . the DVT was terrible, I couldn’t face the day.” Noble, et al (2005). Palliative medicine 19 (3):197-201
CANCER-VTE: THE PATIENT EXPERIENCE • The negative aspects of LWMH “I always bruise on my belly - I did when I was in hospital - doesn’t worry me though” “If Gill (district nurse) was seeing me, no problem, but sometimes this other lass would come round - then it would be bruises” Noble, et al (2005). Palliative medicine 19 (3):197-201
CANCER-VTE: THE PATIENT EXPERIENCE • Semi-structured cross-sectional interview to explore the acceptability of long term LMWH • 14 patients were interviewed • Intention to treat for > 3 months • LMWH for a mean of 42 days at time of interview • Understanding and practicality of LMWH • Positive and negative aspects of LMWH • Included questions exploring attitudes towards DOAC and whether patients would prefer those agents Seaman, et al (2014). Patient preference and adherence 8:453-461.
CANCER-VTE: THE PATIENT EXPERIENCE • If, in the future, there were a tablet available that was worked as well as the injections for cancer-associated blood clots, which would you choose? “It would have to be the tablet. Most definitely” Seaman, et al (2014). Patient preference and adherence 8:453-461.
CANCER-VTE: THE PATIENT EXPERIENCE • What if there were a new tablet that had been tested to confirm that it worked for clots in noncancer patients but had not been tested specifically to see how effective it was in patients with cancer who had blood clots? “I’d opt for the injection…as I said, I don’t mind trying new things, but with reservations. I’ve gone through this now for nearly 11, so I think I know a little bit more than somebody who’s just had had it and I would have to be reassured” Seaman, et al (2014). Patient preference and adherence 8:453-461.
CANCER-VTE: THE PATIENT EXPERIENCE • What if there were a tablet that worked as well as the injection, but we had not way of monitoring whether your blood was too thin or too thick on it? “They phoned up and they said can you come up straight away because you factor Xa is a way too high, and they reduced my dose. If there is no way of monitoring the effect it’s having on your blood, the you don’t know that it’s doing” Seaman, et al (2014). Patient preference and adherence 8:453-461.
PRACTICAL CLINICAL CONSIDERATIONS P-gp CYP 3A Inhibitors (↑exposure): ketoconazole, quinidine, amiodarone, verapamil Inducers (↓ exposure): Rifampin Inhibitors (↑exposure): ketoconazole, clarithromycin, ritonavir Inducers (↓ exposure): Rifampin, St. John’s wort Adapted from Heidbuchel H et al. Europace 2013;15:625-651
PRACTICAL CLINICAL CONSIDERATIONS • Renal insufficiency • Avoid use if Cr Cl < 30 ml/min • Liver dysfunction • Avoid in significant liver dysfunction (i.e.: advanced cirrhosis) • Avoid if transaminases > 2 ULN • Absorption and drug interactions • Not recommended if upper GI malignancy, malabsorption, intractable nausea. • Dose adjustment/avoid if concurrent modulators of CYP 3A4 • Dose adjustment if other concurrent P-glycoprotein substrates
PRACTICAL CLINICAL CONSIDERATIONS DRUG INTERACTIONS: CANCER THERAPIES Short, et al (2014). The oncologist 19 (1):82-93
PRACTICAL CLINICAL CONSIDERATIONS • Severe myelosupression and thrombocytopenia • Not recommended if platelet count < 100K/uL • Avoid if anticipated severe cytopenias, myeloablation • High risk of bleeding patients • Untreated brain metastases (renal cell/melanoma) • Active GI / GU malignancies • Management of bleeding • Consensus measures for hemostasis • Management of Patients on Non-Vitamin K Antagonist Oral Anticoagulants in the Acute Care and Periprocedural Setting: A Scientific Statement From the American Heart Association. Circulation 135 (10):e604-e633. • Idarucizumab (dabigatran) • Andexanet (Xa inhibitors)
CONCLUSIONS • The direct oral anticoagulants may represent a treatment option for cancer related-VTE and an alternative to anticoagulation with VKA. • Until results from cancer population-specific randomized trials are available, LMWH should be the first line treatment for cancer related-VTE. • The precautions and elements of clinical judgment determining if DOACs are safe in cancer are similar to those that determine that decision process in the other adult populations. • Real-world and larger scale studies are necessary to investigate the patient’s experience during the treatment for cancer related-VTE, beyond the outcomes of efficcacy and safety.