Download
1 / 9
90 likes | 300 Views
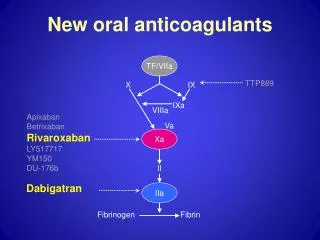
NEW ORAL ANTICOAGULANTS. Dabigatran – direct thrombin inhibitor Rivaroxiban – Xa inhibitor Apixaban – Xa inhibitor.

E N D
NEW ORAL ANTICOAGULANTS Dabigatran – direct thrombin inhibitor Rivaroxiban – Xa inhibitor Apixaban – Xa inhibitor
The implication of the action of all of these new anticoagulants is that because their action is at the end of the coagulation cascade is that they are irreversible in the event of anticoagulant induced bleeding unlike warfarin for which reversal with Prothrombin complex concentrates (PCC) and FFP is possible
Dabigatran • Promoted as not requiring monitoring cf, with warfarin which has multiple drug, dietary and time of ingestion interactions • Has been aggressively promoted by the drug company to GP’s by a “familiarisation” program • Inadequate outline of potential overdose in elderly patients > 75 years and patients with renal impairment • No effective antidote for anticoagulant related bleeding
Rivaroxaban and Apixaban are factor Xa inhibitors only licenced currently as thromboprophylaxis for hip and knee replacement surgery however will be licenced for use in AF in 2013 • Also irreversible in the event of anticoagulant caused bleeding
The only reversal for any of the agents which is proven is the relatively short half life of ~ 15 hours other than haemodialysis which is impractical in the event of acute bleeding • No laboratory monitoring to assess the concentration in plasma is currently available (unlike the INR for warfarin) • Thrombin time can be used to assess the presence of dabigatranin the circulation a normal TT excludes the presence of significant dabigatran levels • APTT/INR are less sensitive
HAPS haematology is currently developing tests to detect the concentration of all 3 of the new anticoagulants however to date there is no correlation with the level of the drug and its anticoagulant effect • Although the drug company claims there are less serious haemorrhagic complications cf. warfarin we have experienced an increased incidence of GI bleeding especially in patients >75yo and with renal impairment. The incidence of cerebral haemorrhage was less but this included patients on warfarin + ASA
The only effective reversal of dabigatran is haemodialysis • The use of FV11a is unproven but has been used in desperate situations • Clotting factors are of no use in bleeding caused by these agents
For a drug to be considered superior to another it should be shown to offer advantages – greater efficacy, ease of use,.safety or cost effectiveness • Compared to warfarin dabigatran causes more GI bleeding, myocardial infarction, has no antidote and costs significantly more than warfarin and there is no laboratory test to monitor adherence
The new anticoagulants are going to have an important role in thromboprophylaxis however the rush by drug companies to promote these expensive new agents has not been balanced by appropriate precautionary advice about the lack of an antidote in the event of bleeding, the lack of laboratory monitoring, the lack of clinical trialsin the patient group most likely tobe prescribed these agents ie, patients > 75 and with renal impairment