Download
1 / 96
970 likes | 1.03k Views
Bioequivalence : some challenges and issues. NATIONAL VETERINARY S C H O O L T O U L O U S E. P.L. Toutain National Veterinary School Toulouse France Informal CVMP/CMDv Paris 2008. [ PHENYTOIN] µg/mL. WEEKS. Change in phenytoin excipients results in epidemic toxicity.

E N D
Bioequivalence : some challenges and issues NATIONAL VETERINARY S C H O O L T O U L O U S E P.L. Toutain National Veterinary School Toulouse France Informal CVMP/CMDv Paris 2008
[PHENYTOIN] µg/mL WEEKS Change in phenytoin excipients results in epidemic toxicity * Bochner F, et al. Proc Aust Assoc Neurol 1973;9:165-70
Non-bioequivalence of various trademarks of enrofloxacin in cow Sumano & al 2001 Dtsch tierärztl Wschr 108 281-320
Aims of the presentation Give an overview on the concept of bioequivalence Discuss some technical points in relationship with the CVMP guideline
Bioequivalence : Definition • Two medicinal products are bioequivalent if their bioavailabilities (rate and extent) after administration in the same molar dose are similar to such degree that their effect and safety will be essentially the same (E.U. for man)
Bioequivalence : The basic assumption • “Similar” overall plasma exposure same effects (efficacy, safety) • is it always true ? • Classical objections • Plasma concentration is not biophase concentration • there is no (univocal) relationships between exposure and effect !
Relevance of plasma concentrations was challenged for ivermectins
DOSE Systemic Effects driven by plasma concentrations Plasma concentrations yes Basic assumption to bioequivalence Is there an univocal relationship between exposure and effect ? yes yes yes Yes Yes Local effects not driven by plasma concentrations Plasma concentrations Yes/No ?
Why to use bioavailability outcomes to demonstrate bioequivalence
Basic assumption to bioequivalence Similar plasma concentration profile same effect ? Why ? Effect = Effect Drug property (efficacy) Emax Emax Dose ED50 + Dose Dose ED50 Hybrid drug and formulation properties (Potency)
Basic assumption to bioequivalence Drug property Clearance EC50 Bioavailability ED50 = Formulation property
Basic assumption to bioequivalence • Similar plasma concentration profile same effect? substance properties Emax Dose Clearance EC50+ Dose F% Effect = Formulation properties
Bioavailability vs Bioequivalence ? = A B injection Analytical approach in vivo approach injection "the cattle column" HPLC column In vivo equivalence Pharmaceuticalequivalence Both HPLC and animal "column" need to be reproducible
Bioequivalence vs. Bioavailability Inference from a trial - Bioavailability No generalization from a subgroup of animal to the population - Bioequivalence If B.E. is demonstrated in a particular subgroup of animals, conclusion should be extended to the whole population unless there is an interaction between formulation and a constitutional factor
Generics: advantages and disadvantages in terms of public health
Generics: Public health perspective • to promote access to medicines through (inter alia) generic competition • generic competition is desirable as it may contribute to significant drug prices decrease • Financial advantage for health care providers • But what about public health perspective for veterinary drugs??
Generic competition for drugs availability:Q1: is it a good news for veterinary medicine especially for antibiotics?
Correlation between community use and the number of trade names for oral-use agents for 6 antibacterial classes in EU High consumption countries Low consumption countries Nb of trade names Nb of trade names
Generic competition for drugs availability: Q2: Is it a good veterinary practice to encourage the use of old antibiotics rather than new ones?
Is it a good veterinary practice to encourage the use of old antibiotics rather new ones? • Traditionally, from a public health perspective, veterinarians are encouraged not to employ new drugs, but rather to use the older antibiotics. • The recommendation whether to choose older rather than new antibiotics was recently challenged on an epidemiological basis (Amyes et al., 2007) and shown to be flawed for quinolones, cephalosporins and carbapenems.
. For three antibiotic classes (quinolones, cephalosporins and carbapenems), it was observed that the less active drugs could be worse at hastening the spread of resistance than more active drugs in the same class. This led the authors to qualify the (WHO) stratagem of recommending the use of old antibiotics as part of microbiological folklore.
Is it a good veterinary practice to encourage the use of old antibiotics rather new ones? • Old antibiotics were developed long time ago and their dosage regimens need to be reassessed (e.g. tetracyclines; quinolones etc.).
Technical issues addressed in the presentation • Bioequivalence: the a priori bioequivalence range • Types of bioequivalence trials • PK, PD vs. clinical trials • Average, population bioequivalence & individual bioequivalence • Interspecies extrapolation • Bioequivalence and drug residues • Male vs. female in bioequivalence trial • Single dose vs. multiple doses • Data analysis: the sequence effect • GLP vs. field conditions
A priori bioequivalence range • These are the two limits ( 1, 2 ) between which the 90% CI interval of the difference or the ratio of the two products should be located in order to accept average B.E. • To be defined by the clinician
Decision procedures in bioequivalence trials BE not accepted BE not accepted 1 2 the 90 % CI of the difference or of the ratio - 20% +20% BE accepted µt Mean of ref formulation
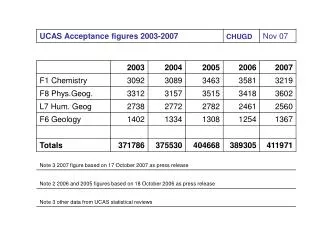
A priori Bioequivalence range:For AUC-difference or AUC-ratio General rule: The 90% confidence interval for this metrics should lie within an a priori acceptance interval: ± 20 % of the reference product (for the difference, untransformed) -20, +25% for the ratio (i.e. 0.8-1.25 for Ln-transformed)
A priori Bioequivalence range:for Cmax-difference or Cmax-ratio 0.70 - 1.30 (untransformed) or 0.70 - 1.43 (Ln-transformed) Wider interval is accepted because Cmax is a single observed extreme concentration
PK/PD relationship to discuss bioequivalence acceptance criteria • A 20% difference for PK has no impact on efficacy • Typically for safe drugs Effect Exposure ∆ = 20%
PK/PD relationship to discuss bioequivalence acceptance criteria • A 20% difference for PK may have an impact on efficacy • Typically for unsafe drugs Effect Exposure ∆ = 20%
A priori Bioequivalence range for drug with a narrow therapeutic index 0.90 - 1.10 (Untransformed) 0.90 - 1.11 (Ln-transformed)
A priori Bioequivalence range for drug with a large therapeutic index • If there are no animal safety or efficacy concerns, is it possible to accept a larger interval (e.g. in case of highly variable drugs)? • Therapeutics vs. equity considerations • Concern about the possibility of study-by-study alteration of approval acceptance criteria
Types of bioequivalence trials Order of preference • Pharmacokinetic • In vitro studies • Pharmacodynamic* • Clinical* * Not considered in draft 4
Clinical or pharmacological endpoint studies to demonstrate BE for systemically acting drugs • Motivations • Blood drug concentration is not quantifiable • Excessive variability in the blood concentration/time profile • Manufacturer/ regulators consider that blood level profiles are irrelevant (or less relevant than a clinical endpoint)
Types of Bioequivalence trialPharmacodynamic endpoints Test Reference 100 % Response A Effect 50 % T and R are not bioequivalent AUC Systemic exposure
Types of Bioequivalence trialPharmacodynamic endpoints Test Reference 100 % Response B Effect 50 % AUC T and R are bioequivalent Systemic exposure
Average vs.population bioequivalencevs. individual bioequivalence
Different types of bioequivalence • Average (ABE) : mean • Population (PBE) : prescriptability • Individual (IBE) : switchability
Average bioequivalence reference test Same mean
Average bioequivalence Average B.E. refers to the location parameters Average B.E. may not be sufficient to guarantee that an individual patient could be switched from a reference to a generic formulation (e.g., more than 50% of subjects may be outside the B.E. range when the average B.E. is actually demonstrated!!!!)
Average bioequivalence • Addresses only mean (center of distribution) but not variability (shape of distribution) • Does not address switchability
Prescribability • Refers to the clinical setting in which a practitioner prescribes a drug product to a patient for the first time • he has no information on his patient • the prescriber needs to know the comparability of the 2 or n formulations in the population population bioequivalence
Population bioequivalencePopulation dosage regimen No Yes Pigs that eat less: Possible underexposure Pigs that eat more Possible overexposure
Individual bioequivalence NO animal-by-formulation interaction YES test reference Address switchability “Test” and “reference” are bioequivalent if the individual subject means and variabilitites are sufficiently similar with regard to AUC and Cmax
Switchability • Refers to the clinical setting in which a practitioner transfers a patient from one drug product to another • We have information on the response of the patient to a particular formulation and clinicians have titrated the dose to reach a particular goal • issue for drug of critical therapeutic categories, for elderly, debilitated patients etc.