Download
1 / 11
110 likes | 220 Views
BME 1300 Problem 1 Newstetter Group. Names of Group. Problem.

E N D
BME 1300 Problem 1Newstetter Group Names of Group
Problem Currently, non-small cell lung cancer is being detected at stages III and IV, causing a five year mortality rate of 86%. This is due to a lack of widespread lung cancer screening methods that have sensitivity and specificity greater than 60%.
Evaluation of Current Methods • Data suggests current screening does not work • High mortality rate • X-rays and sputum cytology - have been proven ineffective in lowering mortality rate • Physical exam - ineffective for screening in early stages due to lack in symptoms • CT Scan – has only been proven effective for high risk patients • Bronchoscopy and biopsy – overly invasive and used primarily for detection
Evaluation of Screening Procedure • Practically no screening done • Patients assessed for risk • Smoker (10 pack years), occupation, family history • If patient is high risk, some will screen, others will wait for symptoms • X-rays followed by CT scans if abnormalities present • CT followed by biopsy/treatment • Sputum occasionally used • Doctors very negative about screening situation
Recommendations for Current Methods • Annual CT for high risk age 55-74 with 30 pack years • Biannual CT for other high risk patients not in 55-74/30 pack year category • Mathematical modeling available soon for other risk groups • Eliminate X-rays for high risk groups • Add PET to CT scan when available • Cell block and smear with sputum cytology
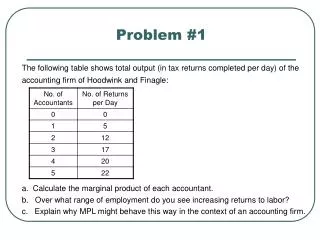
Evaluation Numbers For Future Methods • Grading Scale for Future Methods • 2 x Sensitivity • 2 x Specificity • 1 x Invasiveness • 1 x Risk of Injury from Test Complications • 1 x Practicality (Ease of Analyzing and Collecting Data) • 1 x Implementation (Ease of Achieving Widespread Usage) • Each Ranked 1-5 with 5 being the highest rating
Evaluation Numbers For Future Methods Sputum Biomarkers – 21/40 Methylation of tumor suppression genes 64% sensitivity and specificity PPV = 11.72% Serum Based microRNA– 28/40 Both miR-1254 and miR-547-5p significantly increased in early stage NSCLC 78% sensitivity/75% specificity
Evaluation Numbers For Future Methods Breath Biomarkers – 31/40 Analyzes biomarkers in exhaled breath 84% sensitivity/92% specificity Circulating Cancer Cells – 29/40 • Blood test
Evaluation Numbers For Future Methods Protein Blood Biomarkers – 33/40 • Uses aptamers • 91% sensitivity/84% specificity Bronchoscopy (Epithelial Cells) – 34/40 • Genetic testing of epithelial cells from endobronchial brushings • 95% sensitivity and specificity
Proof of Concept • Given a random population of 100,000 people, 6,950 will be diagnosed with lung cancer. 6,046 of these people will die. With our proposed future method of genetic testing in epithelial cells from endobronchial brushings, our new mortality rate is 53.07%, saving 2,357 lives.
Final Recommendations • Screening methods in distant future • Partial Wave Spectroscopy • Urine Test • Proteomics • Spirometry