Download
1 / 66
660 likes | 820 Views
BIO 169 THE HEART CHAPTER 20. created by Dr. C. Morgan. TOPICS. Introduction and Overview Heart Anatomy The Heartbeat Cardiodynamics. Reference: IPCD Cardiovascular System. Introduction and Overview Objectives. Discuss the work load placed on the heart.

E N D
BIO 169 THE HEART CHAPTER 20 created by Dr. C. Morgan
TOPICS Introduction and Overview Heart Anatomy The Heartbeat Cardiodynamics Reference: IPCD Cardiovascular System
Introduction and Overview Objectives Discuss the work load placed on the heart. Describe the circulatory plan with respect to the heart and lungs. Briefly discuss the definition of arteries, veins, and capillaries.
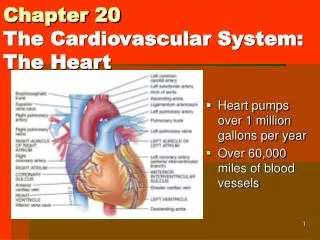
Introduction and Overview The function of the cardiovascular system depends on the heart to develop the hydrostatic pressure which drives the circulation of blood throughout the body. Your heart beats around 100,000 times a day, pumping enough blood to fill forty 55 gallon containers. Multiply those statistics by a lifetime and you will see that an astounding amount of work is accomplished by the heart. Blood flows through a network of vessels that are divided into two circuits, pulmonary and systemic. Vessels are arteries, veins, and capillaries.
Introduction and Overview (cont) HEART LUNGS HEART HEART TISSUES HEART veins carry blood to the heart arteries carry blood away from the heart Fig. 1
TOPICS Introduction and Overview Heart Anatomy The Heartbeat Cardiodynamics
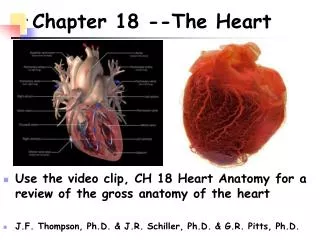
Heart Anatomy Objectives Describe the surface anatomy of the heart. Describe the internal anatomy of the heart. Discuss the heart valves, their location, and function. Characterize the heart wall. Describe the blood supply to the heart muscle tissue.
Heart Anatomy The fist size heart lies in the anterior thoracic cavity, slightly left of the midline, where it is surrounded by connective tissues of the mediastinum. The heart is posterior to the sternum within its own pericardial cavity and surrounded by the pericardium. The parietal pericardium is a dense, irregular connective tissue with an epithelial lining that secretes pericardial fluid into the cavity. Is the pericardium a mucous or serous membrane? The epicardium is the visceral pericardium that adheres to the surface of the heart muscle (myocardium).
Heart Anatomy (cont) base apex Fig. 3 c Fig. 2 b
Heart Anatomy (cont) Base Apex Fig. 2 (c)
Heart Anatomy (cont) Surface fat protects vessels Fig. 3 Left and right atria with auricles Coronary sulcus: a depression between atria and ventricles Interventricular sulcus: between left and right ventricles. 11
Heart Anatomy (cont) The heart wall has three concentric layers that wrap around the atria and spiral within the wall of the ventricles. 3 2 1 squamous epithelium Fig. 4 a
Heart Anatomy (cont) The Myocardium TABLE 1 gap junction communication Ca2+ from ECF and SR Fig. 5 b, c
Heart Anatomy (cont) Cardiac muscle cells are striated, branched, mononucleate, with intercalated discs at intercellular junctions composed of gap, tight, and desmosome junctions. Gap junctions across intercalated disc allows fast, efficient electrochemical communication to form a functional synctium (contracts as one). Cells have many mitochondria due to dependence on aerobic metabolism with energy reserves as stored glycogen and lipids. Mitochondria make up 25% of the cardiac cell volume. Autorhythmic pacemaker cells generate action potentials. Motor neurons of the ANS division modify the heart rate.
Heart Anatomy (cont) The wall structure of the right and left ventricles reflects the different demands placed on them. Right ventricle only has to move blood to nearby lungs. Less vascular length = less pressure needed (thinner wall). Left ventricle must move blood through all the vessels on the arterial side of the systemic circuit which requires much more pressure. Left ventricle has a thicker myocardial wall than the right one. Heart valves prevent backflow (regurgitation) of blood. Papillary muscles and their chordae tendineae keep valve cusps from being pushed into atria.
Heart Anatomy (cont) ridges Frontal section Fig. 6 a
Heart Anatomy (cont) Learn route systemic circuit aorta aortic semilunar valve Lt. ventricle bicuspid valve Lt. atrium venae cavae Rt. atrium tricuspid valve Rt. ventricle pulmonary semilunar valve coronary sinus pulmonary trunk pulmonary arteries lungs pulmonary veins
Heart Anatomy (cont) AV valves open semilunar valves closed diastole Semilunar valves are like 3 little pockets that close the opening when they fill with blood. Fig. 8 a 18
Heart Anatomy (cont) systole semilunar valves open AV valves closed Fig. 8 b 19
Heart Anatomy (cont) Collagenous and elastic fibers in connective tissue wrap around cardiac cells and are continuous with a branching internal network of connective tissue that binds valves in place to form a fibrous skeleton. The fibrous skeleton consists of four bands around the bases of the large vessels and valves to isolate the atria from the ventricles. Connective tissue fibers that bind the cells in place assists in distributing the energy of contraction over the entire myocardium. The blood vessels and nerves are also bound in place by the connective tissue. The elastic fibers cause the myocardium to return to its original size and shape after a contraction.
Heart Anatomy (cont) 1st branches from aorta are left and right coronary arteries RA CAD results from restricted or blocked arteries. Fig. 9 a, b 21
Heart Anatomy (cont) Veins and arteries Fig. 9 c
TOPICS Introduction and Overview Heart Anatomy The Heartbeat Cardiodynamics
Heartbeat Objectives Describe the two types of cardiac cells and their role in contraction of cardiac muscle. Discuss the action potential in cardiac muscle cells. Learn the role of the conducting system of the heart. Learn the components of the electrocardiogram. Relate the electrocardiogram to the contraction cycle. Discuss the origin of heart sounds.
Heartbeat Two types of cells communicate to produce a heartbeat. Contractile cells shorten to pump blood out of the heart. Conducting cells distribute the electrochemical signals that trigger the contraction events in the contractile cells. 99% of the myocardium is composed of contractile cells. Just like in skeletal muscle, an action potential travels along the sarcolemma to trigger the appearance of Ca2+ ions which bind to troponin to reveal actin sites to myosin. Contraction follows but the depolarization-repolarization cycle is 30 times longer in cardiac than skeletal muscle. Because of a long refractory period, tetanus does not occur and the maximum rate is about 200 beats / min.
Heartbeat (cont) -75 mv 250 – 300 msec Fig. 15 a
Heartbeat (cont) twitch myogram The plateau is a major difference between cardiac and skeletal muscle action potentials. no summation or tetanus twitch myogram Fig. 15 b
Heartbeat (cont) ECF source Ca2+ ions that enter the sarcoplasm during the plateau phase of the action potential account for 20% of the total. The SR then releases its Ca2+ into the sarcoplasm. Understanding that the initial ECF calcium source triggers release of the subsequent SR source ions explains the sensitivity of cardiac muscle to ECF calcium ion concentration. Active transport pumps restore the Ca2+ balance. In cardiac muscle, relaxation is underway before the long absolute refractory period ends – no summation or tetanus possible.
Heartbeat (cont) Cardiac muscle is able to initiate its own contractions—a property known as autorhythmicity or automaticity. During a normal contraction cycle, the atria contract before the ventricles. This coordination is possible because of electrochemical signals from specialized muscle cells that do not contract but instead, simply initiate and conduct action potentials to contractile cells. These cells are autorhythmicnodal (pacemaker) and conducting cells respectively. Nodal cells establish the rate; conducting cells distribute action potentials to all of the contractile cells.
Heartbeat (cont) 80 -100 tachycardia = fast rate without neural input 40 - 60 no normal spontaneous depolarization bradycardia = slow rate Fig. 12 a
Heartbeat (cont) spontaneous SA depolarization 75 bpm drift toward threshold Fig. 12 b
Heartbeat (cont) Nodal cells are connected to conducting system cells which in turn branch to all the muscle fibers in the heart. Nodal cells depolarize spontaneously so they set the rate. Pacemaker nodal cells in the sinoatrial (SA) node are usually the first to depolarize at a rate of about 75 / min. The SA node is the pacemaker of the heart. The SA node conducts to the atria and to the AV node located in the floor of the right atrium. The action potential travels to the AV bundle, along the two bundle branches in the interventricular septum, and then are distributed to ventricular muscle cells via the Purkinjesystem of branching, conducting fibers.
Heartbeat (cont) SA node AV node AV bundle bundle branches Purkinje fibers Fig. 13 33
Heartbeat (cont) The AV nodes slows the conduction rate which allows time for the atria to contract. The maximum rate of conduction from the AV node is 230 impulses per minute. The right and left bundle branches are in the interventricular septum. Purkinje fibers conduct action potentials quickly, reaching all ventricular cells within 75 msec. There is a direct path (moderator band) to the papillary muscles so they contract and apply tension to the chordae tendineae before the myocardium contracts.
Heartbeat (cont) P = atrial depolarization ECG tracing of electrical events in the heart QRS = ventricular depolarization T = ventricular repolarization 35
Heartbeat (cont) ECG intervals ECG leads in place Fig. 14 36
Heartbeat (cont) Contraction follows the depolarization events. Atria begin to contract 100 msec after P wave initiation. An upward deflection is seen when the depolarization is moving toward the sensing electrode (patch with attached wire that is connected to the ECG machine). A downward deflection is seen when the depolarization is moving away from the sensing electrode. When there are conduction defects (cardiac arrhythmias), changes in the ECG may be apparent. For example, scar tissue that forms after a heart attack does not conduct so a “detour” occurs to produce an altered tracing.
Heartbeat (cont) Phases of the cardiac cycle Fig. 16 38
Heartbeat (cont) One Blood moves down hydrostatic pressure gradients. 39
Heartbeat (cont) Fig. 17
Heartbeat (cont) The “lubb-dupp” sounds heard through a stethoscope are due to valve closure. The first sound (S1) is due to AV valve closure (ventricular systole) and S2 is heard when the semilunar valves close. Two additional sounds are difficult to hear. S3 is heard as blood fills the ventricles and S4 is associated with atrial contraction. Murmurs are fluid sounds heard due to blood regurgitation into the atria during ventricular systole. Mitral (left AV valve) regurgitation is the most common murmur heard.
Heartbeat (cont) Sites for auscultation of heart sounds Fig. 18 a
Heartbeat (cont) Fig. 18 b
TOPICS Introduction and Overview Heart Anatomy The Heartbeat Cardiodynamics
Cardiodynamics Objectives Present an overview of factors affecting cardiac output. Discuss factors that affect the stroke volume. Describe factors that affect the heart rate. Discuss the cardiac responses to exercise. Describe some abnormal conditions that affect cardiac output.
Cardiodynamics Cardiodynamics refers to the blood movements and forces produced during each cardiac contraction cycle. Both ventricles eject the same amount of blood during systole. Terminology: End-diastolic volume (EDV) = volume of blood in each ventricle at the end of ventricular diastole. End-systolic volume (ESV) = volume in each ventricle at the end of systole. Stroke volume (SV) = volume ejected by each ventricle (SV = EDV – ESV) Ejection fraction = SV as a % of EDV.
Cardiodynamics (cont) Factors affecting CO CO = HR x SV Fig. 23
Cardiodynamics (cont) Stroke volume is affected by changes in the EDV and ESV. EDV is determined by filling time and volume of venous return. Faster heart rates decrease the filling time. Venous return varies with heart rate, blood volume, patterns of peripheral circulation, skeletal muscle activity, and factors that affect venous flow patterns. ESV is affected by preload, contractility of the ventricle, and afterload. *The preload is the volume of blood in the ventricle prior to contraction. Preload sets the length-tension relationship of muscle myofilaments (overlap of actin and myosin).
Cardiodynamics (cont) When the muscle is stretched little (at rest), the myocardium develops a less powerful contraction and the ESV is greater. When you exercise, venous return increases, EDV increases to stretch the myocardium more and ESV decreases because contraction efficiency improves. An overstretched myocardium is inefficient and the ESV is very high (further decreasing venous return and EDV). Within normal limits, the greater the EDV (preload), the greater the stretch on the myocardium, the greater the SV, and the less the ESV. This is the Frank-Starling principle or Starling’s law.
Cardiodynamics (cont) *Contractility is a measure of the force developed by the ventricular myocardium at a given preload. Contractility may be altered by inotropic factors. Drugs that increase contractility exert positive inotropic effects usually by stimulating Ca2+ movement into the sarcoplasm or prolonging its presence there. Drugs that decrease contractility exert negative inotropic effects usually by blocking Ca2+ movement into the sarcoplasm or decreasing metabolism. The ANS, hormones, and ECF ion concentrations all affect contractility.