Download
1 / 67
670 likes | 836 Views
LC-MS Determination of Bile Acid-Sulfates As Biomarkers for Liver Function. Yazen Alnouti, Ph.D Assistant Professor Department of Pharmaceutical Sciences University of Nebraska Medical Center. BA Enterohepatic Recirculation. 95%.

E N D
LC-MS Determination of Bile Acid-Sulfates As Biomarkers for Liver Function Yazen Alnouti, Ph.D Assistant Professor Department of Pharmaceutical Sciences University of Nebraska Medical Center
BA Enterohepatic Recirculation 95% Under normal conditions, BAs are contained within the enteroheaptic system, spill over into blood is minimum, and urinary excretion is negligible
22 21 20 23 18 12 17 24 11 13 19 16 14 15 1 9 8 2 10 3 5 7 4 6 Backbone Structure
Eras of Interest in BAs Lipid Absorption/Cholesterol Elimination Cytotoxicity Genotoxicity Cholestasis/ Liver Toxicity Colon Cancer Treatment of hepatobiliary diseases Signaling Molecules (Hormones): nuclear receptors ligands • BA Homeostasis (Cholestasis) • Glucose Homeostasis (Diabetes) • Energy Homeostasis (Metabolic Syndrome)
Missing with BA Homeostasis Can be the Kiss of Death • Bile/Liver = 64 mM/0.45 mM = 150 fold • Liver/Plasma = 0.45 mM /1.2 mM = 400 fold • Bile/Plasm = 64 mM /1.2 mM = 60,000 fold
Pathologic Effects Physiologic Functions BA Homeostasis BA homeostasis is tightly controlled by nuclear receptor-mediated mechanisms which up- and/or down-regulate target genes involved in BA: i) Synthesis ii) Transport iii) Metabolism
PAPS PAP SULT2A1 - BA Homeostasis/Sulfation • Sulfate-conjugates carry a permanent negative charge (pKa of sulfate moiety < 1) • Efficient pathway of BA detoxification: • i. Decrease intestinal absorption • ii. Increase fecal excretion • iii. Increase urinary excretion • iv. Decrease toxicity
BA Sulfation in Humans • Under normal conditions, total BAs excreted in urine is <1 mMole/day (40-70% sulfated), total BAs in plasma < 3 mM (<10% sulfated), up to 4% of BAs in bile are sulfated • LCA (mono-hydroxy BA) is almost exclusively present in the sulfated form, whereas CA (Tri-hydroxy BA) is mostly present in the unsulfated form. • In hepatobiliary/cholestatic diseases, due to the impairment of biliary excretion, BAs in blood, tissues, and urine increase • - Amounts of BA-sulfates also increase In bile, urine (>100x), plasma • - Concluded that BA sulfation is induced during hepatobiliary diseases to protect against BA accumulation and toxicity • - % of BA-sulfates/BAs decrease/increase ?! (missing)
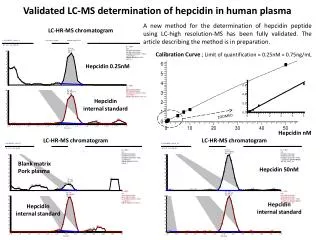
Marked Variation on Data on BA-Sulfates in Health & Disease Alnouti Y. Toxicol Sci. 2009 Jan 8. [Epub ahead of print]
Analysis of BA-Sulfates • The variation in Data on BAs and BA-sulfates is largely due to the analytical techniques used to quantify them • BA-sulfates are desulfated during sample preparation, then unconjugated BAs are quantified by: • i. 3-a-OH-steroid dehydrogenase (3aHSD) • ii. GC/GC-MS • iii. LC-UV/Fluorescence/(3aHSD) • iv. LC/MS-(FAB, ESI) • - These methods are not direct and they lack specificity, sensitivity, validation, and/or dynamic range
Linear IT C18-LC ESI UPLC-MS/MS
Representative Chromatogram of Bile Acid Mixture G-CA G-CA 2 1. G-UDCA 2. G-CDCA 3. G-DCA 3 1 G-LCA 2 1 1. T-MCA 2. T-CA Intensity 1 3 1. T-UDCA 2. T-CDCA 3. T-DCA 2 T-LCA 2 1. a-MCA 2. b-MCA 3. CA 3 1 1. T-UDCA 2. T-CDCA 3. T-DCA 2 3 1 LCA 2H4-G-CDCA (+IS) 2H4-CDCA (-IS) Time (Min)
Current + Future BA-related Research in my Lab • LC-MS/MS method for the quantification of BA-sulfates • . MS conditions: direct vs. indirect (scanning) • . Sample Preparation: SPE, PP, LLE..etc • . Chromatography: column, mobile phase, wash..etc • . Validation: accuracy, precision, stability..etc • SULT2A1 Cell Line: in vitro kinetics of sulfation of BAs and others! • Synthesis/Biosynthesis of BA-Sulfate standards • - Hepatotoxicity of endothelin receptor-2 antagonists
Significance • Need-Driven: • There is a critical need for direct, sensitive, valid, specific, simple, and fast bioanalytical methodology for the quantification of BAs and BA-sulfates in biological matrices • ii. Hypothesis-Driven: • BA-sulfates can be used as a biomarker for liver function in hepatobiliary diseases
Specific Aims i. Develop and Validate a rapid, specific, and sensitive LC-MS/MS method to quantify individual BA and BA-sulfates ii. Bile, urine, plasma analysis from patients with hepatobiliary diseases (liver transplant) iii. Correlation Analysis of individual BA and BA-sulfates
Novelty i. No direct and valid methodology to quantify specific BA sulfates in biological fluids and tissues ii. No selective biomarker available to diagnose and predict the outcomes of liver disease treatment/transplant
Predicted Outcomes/ Fit to COBRE • Development and validation of a novel rapid bioanalytical methodology for the analysis of BA-sulfates in biological matrices, which will be available for scientists in BA research • The application of this methodology is expected to lead to the discovery of a novel biomarker for liver function • The biomarker which can be used is the diagnosis and treatment of several hepatobiliary diseases and/ or liver transplant
Bile acid toxicity in man: hepatobiliary • Accumulation of intermediates in bile acid biosynthesis in hepatocytes because of inborn enzyme deficiencies • Elevated concentration in hepatocytes because of defective canalicular transport (BSEP deficiency, cholestasis of pregnancy) • Elevated concentrations in cholangiocytes because of bile duct obstruction (PBC, PSC)
Foreläsningar i Djurkemien, 1808 “The function of bile in the body is to digest chyme in the duodenum. The bile substance remains in solution to be resorbed and used again.”
Eras of Interest in BAs Lipid Absorption/Cholesterol Elimination Cytotoxicity/Genotoxicity Cholestasis/Liver Toxicity Colon Cancer Treatment of hepatobiliary diseases Signaling Molecules (Hormones): nuclear receptors ligands • BA Homeostasis (Cholestasis) • Glucose Homeostasis (Diabetes) • Energy Homeostasis (Metabolic Syndrome)
Bile Acids Are Nuclear Receptor Ligands
Bile Acids Are Very Different Lipophylicity (membrane destruction): LCA>>>CA DCA causes cholestasis, whereas CA causes hypercholeresis Cytotoxicity/genotoxicity: LCA>>>CA Hepatobiliary Toxicity: UDCA treats gallstone, whereas LCA is very cytotoxic FXR ligands: CDCA>>>LCA PXR, VDR ligands: LCA>>>CDCA
22 21 20 23 18 12 17 24 11 13 19 16 14 15 1 9 8 2 10 3 5 7 4 6 Backbone Structure
21 22 20 26 23 18 BAS BAT 25 24 12 17 19 11 13 16 27 14 15 1 9 2 10 8 7 5 3 6 4 BA Synthesis Classic/Neutral CYP8B1 7-OH- Cholesterol Intestine CA CYP7A1 DCA glycine/taurine Conjugates Cholesterol Intestine CYP46A1, 25 CYP27A1 LCA CYP7B1 7, 27-DiOH-Cholesterol CDCA Oxysterol CYP39A1 Alternative/Acidic UDCA (3a, 7b-di-OH) Bears MCA (3a, 6a/b,7a/b-tri-OH) Rodents
BA Metabolism/Homeostasis Hydroxylation Conjugation Transporters Synthesis
CFTR Cl- NTCP OATP? BA OA OCT OC MDR2/3 MDR1 Cl- AE PS HCO3- Bile flow FIC1 PC PL BA ASBT H2O Cl- Ch OA AQP BSEP BA ABCG5/8 Cholangiocyte MRP2 Hepatocyte MRP4 Figure from Alan F. Hofmann, University of California Sann Diego
Bile acid toxicity in man: hepatobiliary • Accumulation of intermediates in bile acid biosynthesis in hepatocytes because of inborn enzyme deficiencies • Elevated concentration in hepatocytes because of defective canalicular transport (BSEP deficiency, cholestasis of pregnancy) • Elevated concentrations in cholangiocytes because of bile duct obstruction (PBC, PSC)
Hepatobiliary Bile Acid Toxicity in Experimental Animals • Increased concentration of lithocholic acid (LCA) because of feeding CDCA (or UDCA) and defective detoxification of LCA (mouse, rhesus monkey and baboon) • Elevated concentrations of simple BA micelles in bile causing cholangiocyte destruction because of absent phospholipid in bile (MDR2 deficiency) (mice) • Increased concentration of deoxycholic acid and its 3-oxo derivative because of taurocholate feeding cause lethality in guinea pig Figure from Alan F. Hofmann, University of California Sann Diego
Drugs can inhibit bile acid transporters: a “kiss of death” • Assay: • Polarized monolayers in which NTCP and BSEP have been transfected • Testing of drugs for inhibition of uptake via NTCP or canalicular secretion via BSEP • Fluorescent bile acids for high throughput screening (laboratory of Yuichi Sugiyama, University of Tokyo)
How BAs Are Quantified? 3-a-OH-steroid dehydrogenase (3aHSD) GC/GC-MS LC-UV/Fluorescence/(3aHSD) LC/MS-(FAB, ESI)
Enzymatic Determination of 3α-hydroxy Bile Acids HPLC of human biliary bile acids Origins: Talalay, Iwata and Yamasaki, Javitt, Palmer
There is a critical need for valid, accurate, and simple analytical methodology for the quantification of BAS and their metabolites in biological matrices
Triple Quadrupole C18-LC ESI LC-MS/MS
Triple Quadrupole C18-LC ESI LC-MS
Method Development • MS Conditions • Chromatography Conditions • Sample Preparation • Method Validation
MS Conditions Compound Dependent Parameters • Capillary Voltage: 3 kV • Cone Voltage: Compound dependent • Extractor Voltage: 4 V • RF lens: 0 V • Source Temperature: 120 C° • Desolvation Temperature: 375 C° • Desolvation Gas Flow: 500 L/hr • Cone Gas Flow: 65 L/hr • Collision Energy: Compound dependent • Polarity: Compound dependent
MS/MS Transitions _ _ +
Final LC Conditions The mobile phase consisted of 5% acetonitrile (ACN) in methanol (MeOH) (mobile phase A) and 7.5 mM ammonium acetate adjusted to pH 4 using acetic acid (mobile phase B) at a total flow rate of 0.3 ml/min.
Representative Chromatogram of Bile Acid Mixture G-CA G-CA 2 1. G-UDCA 2. G-CDCA 3. G-DCA 3 1 G-LCA 2 1 1. T-MCA 2. T-CA Intensity 1 3 1. T-UDCA 2. T-CDCA 3. T-DCA 2 T-LCA 2 1. a-MCA 2. b-MCA 3. CA 3 1 1. T-UDCA 2. T-CDCA 3. T-DCA 2 3 1 LCA 2H4-G-CDCA (+IS) 2H4-CDCA (-IS) Time (Min)
Representative Bile Chromatogram G-CA 1. G-UDCA 2. G-CDCA 3. G-DCA 2 3 1 G-LCA 2 1 1. T-MCA 2. T-CA 2 1. T-UDCA 2. T-CDCA 3. T-DCA 1 3 T-LCA 2 1. a-MCA 2. b-MCA 3. CA 3 1 1. T-UDCA 2. T-CDCA 3. T-DCA 2 1 3 LCA 2H4-G-CDCA (+IS) 2H4-CDCA (-IS) Intensity Time (Min)
Quantification of Endogenous Analytes is Hard There is no blank matrix to construct a calibration curve?! • Labeled standards of each analyte • Method of standard addition • Matrix stripping
Sample Preparation • Liver: Alkaline-ACN protein precipitation • Plasma: ACN protein precipitation • Urine: Solid Phase Extraction (SPE) • Bile: Solid Phase Extraction (SPE)
Extraction Recoveries(extraction efficiency + matrix effect/suppression)
Method Validation • Limit of detection (LOD) & quantification (LOQ) • Specificity & carry over • Stability (bench top, freeze/thaw, autosampler) • Matrix effect • Dynamic range • Goodness of fit • Accuracy and precision • Ruggedness
BA Calibration Curves T-DCA G-CA T-MCA G-UDCA MDCA G-CDCA CA G-DCA UDCA T-CA T-UDCA CDCA T-CDCA UDCA
Applications • Control Mice: BA profiling in mouse tissues and fluids • Male vs. female mice • Bosentan toxicity (Jaeschke) • FXR null mice (Guo) • BAs toxicity/dose response (Klaassen)