Download
1 / 11
110 likes | 234 Views
EBP & Tracheostomy: JUST DO ing IT. NSW Speech Pathology EBP Network EBP Extravaganza 6 December 2006 Emma Clifton Senior Speech Pathologist Blacktown & Mt Druitt Hospitals (02) 9881 8612 Emma.Clifton@swahs.health.nsw.gov.au. Session Outline.

E N D
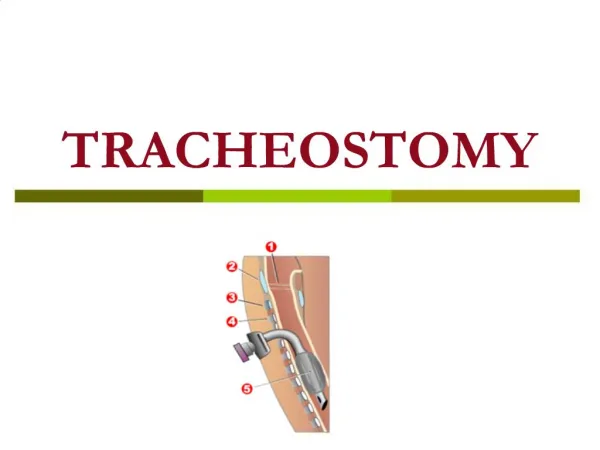
EBP & Tracheostomy:JUST DO ing IT NSW Speech Pathology EBP Network EBP Extravaganza 6 December 2006 Emma Clifton Senior Speech Pathologist Blacktown & Mt Druitt Hospitals (02) 9881 8612 Emma.Clifton@swahs.health.nsw.gov.au
Session Outline • Tracheostomy CATs & CAPs … what’s new? • Tracheostomy EBP & clinical practice … an emerging relationship • Tracheostomy EBP & the workplace … JUST DO ing IT
Tracheostomy CATs & CAPs … What’s new? • Clinical Question • In non-ventilated patients with tracheostomy tubes, does occlusion with a Passy Muir Speaking Valve (PMSV) or a one-way valve reduce aspiration? • CAPs • Dettelbach et al 1995 • Elpern et al 2000 • Gross et al 2003 • Stachler et al 1996 • Suiter et al 2003 • Clinical Bottom Line • Occlusion will not always eliminate aspiration, but it can reduce aspiration with thin fluids • Modified Barium Swallow (MBS) recommended due to high silent aspiration risk • Changing TDG Clinical Practice • It is not assumed that if aspiration is occurring that it will be eliminated by use of a PMSV/one-way speaking valve, but highlights that more objective assessment is frequently indicated
Tracheostomy CATs & CAPs … What’s new? • Clinical Question • In non-ventilated patients with head/neck cancer and tracheostomy tubes, does occlusion reduce aspiration? • CAPs • Leder et al 1998 • Logemann et al 1998 • Muz et al 1989 • Stachler et al 1996 • Clinical Bottom Line • Occlusion can reduce aspiration with some of these patients, possibly due to changes in swallowing bio-mechanics • Occlusion immediately post-surgery ineffective in reducing aspiration • MBS recommended
Tracheostomy CATs & CAPs … What’s new? • Clinical Question • In non-ventilated patients with tracheostomy tubes, does digital occlusion reduce aspiration? • CAPs • Leder et al 1996 • Leder et al 2001 • Logemann et al 1998 • Clinical Bottom Line • Occlusion does not appear to not make a significant difference in eliminating aspiration • MBS recommended
Tracheostomy CATs & CAPs … What’s new? • Clinical Question • In patients with tracheostomy tubes, is the Modified Evans Blue Dye Test (MEBDT) an effective clinical indicator in determining aspiration? • CAPs • O’Neill-Pirozzi et al 2003 • Belafsky et al 1999 • Belafsky et al 2003 • Brady et al 1999 • Donzelli et al 2001 • Thompson-Henry & Braddock 1995 • Peruzzi et al 2001 • Clinical Bottom Line • MEBDT may not be sensitive enough to detect trace aspiration, both • high false -ve rates - when suctioned, up to ~ 46% of the time no blue dyed material will be returned when aspiration has occurred under FEES and MBS • high false +ve rates - when suctioned, up to ~ 20% of the time return of blue dyed material does not actually represent aspiration of item tested eg. was it puree? OR was it saliva? • Note also that food/fluid/saliva can be suctioned from the supraglottis rather than aspirated material • Changing TDG Clinical Practice • Clinical Pathways for RPA and Liverpool Hospital no longer state that the MEBDT is essential in the Speech Pathologist’s toolbag
Tracheostomy CATs & CAPs … What’s new? • Clinical Question • In non-ventilated patients with tracheostomy tubes, is capping indicated for safe and effective decannulation? • CAP • Thompson-Ward et al 1999 • Clinical Bottom Line • Down-sizing + capping and 24-48 hrs cuff deflation both effective • < 3% re-cannulation with both protocols • 24-48 hrs cuff deflation more efficient in facilitating earlier decannulation and reducing medical costs • Changing TDG Clinical Practice • Capping not being a ‘must-do’ before safe and effective decannulation
Tracheostomy CATs & CAPs … What’s new? • Clinical Question • Is it safe to feed patients with the tracheostomy cuff inflated? • CAPs • Pinkus 1973 • Clinical Bottom Line • Patients with tracheostomy tubes should be fed non-orally due to aspiration risk … TDG currently re-visiting ...
Tracheostomy EBP & clinical practice … An emerging relationship Other considerations: • The time factor … • to have discussions • to ‘let go’ of tools and beliefs • to apply the evidence • Some clinical questions where you would expect many papers, to be out there are not • Robustness of studies in existence
Tracheostomy EBP & the workplace … JUST DO ing IT • Having CAPs and CATs with us when seeing patients • Utilising the tracheostomy listserve • Liaising with Librarians for automatic notification of new articles for our CIAP search • Time managing for EBP • Being aware of what exactly is out there, so as to be able to assert view from a position of strength
References • NSW Speech Pathology EBP Network: Tracheostomy Education for NSW Speech Pathologists