Download
1 / 24
240 likes | 547 Views
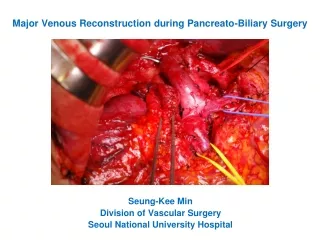
Biliary Injuries During Laparoscopic Cholecystectomy. Aaron M. Williams, M1 University of Kentucky College of Medicine MIS Elective. Focus. Overview of LC and Biliary Injury Laparoscopic Cholecystectomy (Procedure) Biliary Anatomy Biliary Injury Mechanisms and Classification

E N D
Biliary Injuries During Laparoscopic Cholecystectomy Aaron M. Williams, M1 University of Kentucky College of Medicine MIS Elective
Focus • Overview of LC and Biliary Injury • Laparoscopic Cholecystectomy (Procedure) • Biliary Anatomy • Biliary Injury Mechanisms and Classification • Management of Bile Duct Injury • Prevention
History of LC • Widespread acceptance in early 1990’s • “Gold Standard” treatment for gallbladder removal • Approx. 750,000 LCs are performed each year in the U.S. General advantages of LC—MIS approach • Reduced hospitalization • Improved recovery time • Decreased PO pain • Improved cosmesis • Reduced cost
The Problem • LC has been associated with a higher incidence of IA bile duct injuries • LC—0.4 to 0.8% • Traditional OC—0.1-0.3% • Association: • Increased mortality and morbidity • Reduced long-term survival • Reduced quality of life • Infrequent—but among the leading sources of malpractice claims against surgeons. • Between 34% and 49% of surgeons are expected to cause such an injury during their career. • Awareness and preventative methods are of clinical importance to surgeons.
Risk Factors and Mechanism • Risk Factors • Anatomical • Anatomical variations (biliary and vasculature) • Bleeding, scarring, obesity • Laparoscopic • Lack of Depth Perception, Tactile Feedback, Full Manual Maneuverability • Improper surgical approach • Improper Lateral retraction (insufficient or excessive) • 0 degree scope • Approach plane too deep • Lack of conversion to OC during difficult cases
Mechanism of injury • Initially…Surgeon’s Learning Curve –Steady • Anatomical Misidentification: excision, incision, or transection of biliary anatomy • Injuries:common bile duct, common hepatic duct, right and left hepatic ducts, right hepatic artery, ducts draining hepatic segments • Anatomical variations (biliary and vasculature) • Electrocautery, thermal injury: stricture of CBD or hepatic ducts, bile leak • Mechanical trauma: stricture of the biliary ducts, bile leaks • Improper surgical approach
Operating Room Setup • Reverse Trendelenburg (30 degrees) with left arm out at 90 degrees relative to the body’s axis • Titled left 15 degrees after optical trocar placement
Instrumentation • (1)--10 mm optical trocar (umbilical region) • (2)--5 mm operating trocars (subcostal ports) • - (1)--5 mm operating trocar (epigastric region) • - 10 mm 30 degree laparoscope • Clip Applier • Straight Dissector • Metzenbaum Scissors • Grasper(s) • Scalpel and Suture • L-hook electrocautery • Suction-irrigation device (5mm and 10mm) • Probe • Extraction Bag • Cholangiogram
Epigastric region, below XP Trocar Placement Subcostal, Mid-Clavicular Umbilical region Mid-A, between 12th rib and ilium
BiliaryAnatomy a. Right hepatic duct. b. Left hepatic duct. c. Common hepatic duct. d. Portal vein. e. Hepatic artery. f. Gastroduodenal artery. g. Right gastroepiploic artery. h. Common bile duct. i. Fundus of the gallbladder. j. Body of the gallbladder. k. Infundibulum. l. Cystic duct. m. Cystic artery. n. Superior pancreaticoduodenal artery. Schwartz’s Principles of Surgery, 8th Ed.,McGraw-Hill Companies, 2005.
Remember…Mechanism of injury • Anatomical Misidentification: excision, incision, or transection of biliary anatomy • Injuries:common bile duct, common hepatic duct, right and left hepatic ducts, right hepatic artery, ducts draining hepatic segments • Anatomical variations (biliary and vasculature) • Electrocautery, thermal injury: stricture of CBD or hepatic ducts, bile leak • Mechanical trauma: stricture of the biliary ducts, bile leaks
Classic Laparoscopic Injury --Mistaking the common bile duct for the cystic duct
Thermal Injuries • Inappropriate use of electrocautery near biliary ducts • May lead to stricture and/or bile leaks • Mechanical trauma can have similar effects Lahey Clinic, Burlington, MA.1994
Strasburg Classification • Type A Cystic duct leaks or leaks from small ducts in the liver bed • Type B Occlusion of a part of the biliary tree, almost invariably the • aberrant right hepatic ducts • Type C Transection without ligation of the aberrant right hepatic • ducts • Type D Lateral injuries to major bile ducts • Type E Subdivided as per Bismuth classification into E1 to E5
Strasburg Classification, cont’d • E: injury to main duct (Bismuth) • E1: Transection >2cm from confluence • E2: Transection <2cm from confluence • E3: Transection in hilum • E4: Seperation of major ducts in hilum • E5: Type C plus injury in hilum
Lau classification (2007) • Type 1 Leaks from cystic duct stump or small ducts in liver bed • Type 2 Partial CBD/CHD wall injuries without (2A) or with (2B) tissue loss • Type 3 CBD/CHD transection without (3A) or with (3B) tissue loss • Type 4 Right/Left hepatic duct or sectoral duct injuries without (4A) or with (4B) tissue loss • Type 5 Bile duct injuries associated with vascular injuries CBD, common bile duct; CHD, common hepatic duct.
Lau Possible Mechanisms 1– Insecure closure of cystic duct; too deep dissection into gallbladder bed 2 – Incision of CBD instead of cystic duct for operative Cholangiogram; Clipping of CBD but recognized; Laceration of cystic duct/CBD junction; Diathermy injury to CBD/CHD 3 – CBD mistaken as cystic duct, with CBD/CHD transected or Resected; Diathermy injury 4 – Right HD or sectoral duct mistaken for cystic duct 5 – Right hepatic artery mistaken for cystic artery; Diathermy or clip injuries to right hepatic artery
Intraoperative Detection • Only 25-33% of injures are recognized intraoperatively • If experienced, convert to Open Procedure and perform Cholangiography (determine extent of injury) • If not experienced, perform the cholangiogram laparoscopically with intent of referring patient (placement of drains) • Consult an experienced hepatobiliary surgeon Quicker the repair, the better the outcome!!! • Acute Management • Biliary catheter for decompression of biliary tract and control of bile leaks • Percutaneous drainage of intraperitoneal bile collection
Post-Operative Detection Plan • Controlling sepsis, establish biliary drainage, postulate diagnosis, type and extent of the bile duct injury. • Broad-spectrum antibiotics • No need for an urgent laparotomy. Biliary reconstruction in the presence of peritonitis results a statistically worse outcome in patients. • No need for urgent with reconstruction of the biliary tree. The inflammation, scar formation and development of fibrosis take several weeks to subside. • Reconstruction of the biliary tract is best performed electively after an interval of at least 6 to 8 weeks.
BDI Management • Patient presents with… • Vague abdominal pain, nausea, fever, jaundice, vomiting • Investigation • Ultrasonagraphy and CT (ductal dilatation and intra-abdominal collection) • Cholangiogram • ERCP—biliary anatomy and assess the injury • PTC—define biliary anatomy proximal to injury • MRCP—noninvasive (can miss minor leaks) • MR angiography—vascular injuries
Management of Bile Duct Injuries, Cont. • Corrective Treatment (Lao) • Endoscopic stenting for strictures • T-tube placement for minor lacerations • Primary duct-to-duct repair only if tension free anastomosis available • Biliary anastomosis with jejunal loop for major excisional injuries
Preventative Measures (Lao) • Attention to operative details (insufficient close or deep plane) • Stasberg’s critical view of safety • Appropriate Handling of Gallbladder • Careful use of diathermy • Recognition of Biliary and Vasculature Anomalies
Bibliography • Schawartz’s Principles of Surgery, 8th ed., The McGraw-Hill Companies, 2005. • Blumgart L.H. Surgery of the Liver, Biliary Tract, and Pancreas, 4th edition. Saudders Elseiver. 2007. • Nagral S. Anatomy relevant to cholecystectomy. J Min Acess Surg 2005; 1:53-58. • Haney C. and Pappas T. Management of Common Bile Duct Injuries. Operative Techniques In General Surgery. January 2008. 175-184. • Archer et al. Bile Duct Injury During Laparoscopic Cholycystectomy: Results of a National Survey. Annals of Surgery. Volume 234, No 4, 549-559. • Wudel, James et al. Bile Duct Injury Following Laparoscopic Surgery: A Cause for Continued Concern, The Am Surg, June 2001, 67:557-565. • Massarweh N. and Flum D. Role of Intraoperative Cholangiography in Avoiding Bile Duct Injury. J. Am. College of Surgeons. Vol 204, No. 4. April 2007. • Lau et. All. Management of Bile Duct Injury After Laparoscopic Cholecystectomy: A Review. ANZ J Surg 80 (2010) 75–81 • Mortele, Koenradd et al. Anatomic Variants of the Biliary Tree: MP Cholangiographic Findings and Clinical Applications, Am J of Roent, August 2001; 177:389-394. • Ragozzino, Alfonso et al. Value of MR Cholangiography in Patients with Iatrogenic Bile Duct Injury After Cholecystectomy. Am J of Roent, December 2004; 183:1567-1572. • Khalid, Tahir et al. Using MR Cholangiopancreatography to Evaluate Iatrogenic Bile Duct Injury, Am J of Roent, December 2001; 177:1347-1352.