Download
1 / 18
190 likes | 393 Views
Regulation of Kidney Function and Water Homeostasis: 3/24 and 3/26. Dialysis: how and why? Urination: how and why? How do diuretics work? What are the clinical qualities we associate with urine? Why is the kidney important for the removal of toxin and sensitive to toxicity of toxins?

E N D
Regulation of Kidney Function and Water Homeostasis: 3/24 and 3/26 • Dialysis: how and why? • Urination: how and why? • How do diuretics work? • What are the clinical qualities we associate with urine? • Why is the kidney important for the removal of toxin and sensitive to toxicity of toxins? • How does the kidney autoregulate its function? • Why is the juxtaglomerular apparatus so important for autoregulation? • What is the function of the renin-angiotensin-aldosterone system? • How does ANF protect the heart?
Why is it important to remember that urination is partly controlled by the parasympathetic nerves? Spinal cord injury recipients may still have partial local control over bladder function in spite of the injury because the reflex does not “need” the brain!
Where/How do diuretics work? Thiazides: Furosemide: Aldosterone antagonists: Caffeine: RedBull? Mannitol/Glucose: Acidosis: Alkalosis: Proteinuria: If polar molecules stay in the filtrate your urine volume increases! With this in mind why do diuretics drugs make you urinate? What effects would diuretic drugs have on your blood volume, blood pressure, ventricular work, edema, physical appearance and mental functions?
Diuretics • Thiazides: Inhibit Na+ reabsorption in the DCT • Furosemide: inhibits the Na+-K+-Cl- symport in the ascending loop of Henle • Aldosterone antagonists: block effects of aldosterone (block Na+ reabsorption) • Caffeine: Dilates afferent arterioles (GFR) • Osmotic diuretics: mannitol/glucose, acidosis, alkalosis, proteinuria
How do we describe the qualities of urine and glomerular filtrate? • Color: Urochromes, Hematuria, cloudy or with precipitates • Volume: Anuria- none, Oligouria-0.5l/day, Polyuria/diuresis- +2l/day • Odors and disease? Fresh(Pungent), Fruity(Diabetes), Mousy(PKU) Bacteria divide in bladder and create ammonia Ammonia gives it a distinct smell if infected Urine Qualities: pH of urine=4.5-8.2 (it may hurt to urinate if pH is acidic): Osmolarity= 50(clear) - 1,200 mOsm (dark yellow and dehydrated) Specific Gravity= 1.001-1.028g/ml (dark yellow and dehydrated) Pyuria”pus”: Why do bacteria generally not reside inside the kidney (pyelitis) except if you are unable to produce glomerular filtrate? Why does the presence of glucose in the urine of a diabetic typically herald infection with bacteria?
Why is the kidney SO very sensitive to some types of toxin? Concentration of filtrate/urine may effect toxicity of a molecule to kidney itself. • Consider what happens if the wastes/toxins in 180L of GFR is concentrated into1 L of urine. This means the relative concentration of a possible toxin in the urine could increase X180 times! • Concentration effects may create a “Renal Calculus”(stone) when molecules begin to precipitate or crystallize. Why can propylene glycol (antifreeze) cause massive kidney failure (death) if large amounts are consumed? • Antifreeze is converted to oxalic acid by the liver (low toxicity). • Reabsorption of water from GFR increase oxalic concentration by up to X180 times! 180 L GFR 1 Liter of urine so, less toxic Oxalic Acid from the blood Precipitates as sharp crystals! • Effect most pronounced in collecting duct where oxalic acid precipitates as RAZOR SHARP CRYSTALS that slice their way as they go to the ureter, bladder, etc. Causes MASSIVE RENAL FAILURE! Why is the promotion of massive hydration good for persons with PEG poisoning?
TUBULAR SECRETION IS ONE WAY THE KIDNEY CAN ACTIVELY REMOVE MATERIALS FROM THE CAPILLARY THAT WERE NOT FILTERED. • PCT reabsorbs some filtered waste by accident and pumps re-remove these wastes back to the PCT (secretion). • Charges on filtered molecules tend to keep filtered molecules from being reabsorbed through non-polar plasma membranes. • Trick: if you want to remove a toxin or drug, attach a polar group to it like a sulfate, carboxyl or amine • The liver is very important for drug/toxin removal in the kidney in this regard. • Urine pH can also be important for removal of compounds because some compounds become less polar (better reabsorption) when the urine pH is acidic or basic. • Consider the efforts taken by persons to modify urine pH in order to pass urinalysis and drug testing!
STRICT AUTOREGULATION keeps the GFR at a constant 120 ml/minute and renal blood flow at an amazingly constant 1,300 ml/min under a wide range of conditions that include huge differences in blood pressure and even the loss of a kidney. HOW? Flow ml/minute GFR RPF RBF 120 700 1300 Arterial blood pressure “too” high Arterial blood pressure “too” low Range of healthy GFR Autoregulation 20 70 120 200 Mean Arterial Blood Pressure (mmHg)
Creatinine is an end product of phosphocreatine metabolism in the body that appears in blood/urine.. 1) Creatine or phosphocreatine degrade to form creatinine. 2) Blood carries creatinine to glomerular corpuscles. 3) Creatinine is filtered and appears in GFR (if you have GFR!). 4) Creatinine is not reabsorbed so it stays in urine. 5) Less GFR Less ability to remove creatinine from blood and blood levels increase 6) High blood creatinine can indicate that kidney failure has or is starting to occur. NO GFR no salt or water volume control Creatinine leaves the body in the urine, but you only make urine if you have a GFR. So if you have no GFR-No creatinine is removed from the blood
THE KIDNEY HAS AN AMAZING ABILITY TO SELF-REGULATE ITS FUNCTION AND MAINTAIN GFR=125 ml/min! The importance of autoregulation to transplant patients should be self-evident! There are no nerves entering and donor kidney continues to work great (if you can find a donor)! Indicators of dangerous hypovolemia in the circulatory system: Low BP, Low Na+ or Low GFR Tubuloglomergular Feedback and Juxtaglomerular Apparatus Lets you monitor the quality of filtrate as it enters the collecting duct and modify GFR to maintain homeostasis. There are three Players Involved! Juxaglomerular Cells: are smooth muscle cells around the afferent/ efferent arterioles that constrict/dilate to control GFR. They can also initiate renin cascade if blood pressure is TOO LOW • Also: Sympathetic N.S. can directly stimulate JG cells/renin during stress and increase blood pressure/conserve water Macula Densa Cells: Epithelial cells of DCT monitor GFR and Osmolarity and stimulate JG cells Mesangial Cells: May help JG/MD cells communicate.
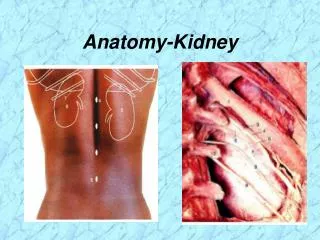
The Juxtaglomerular Apparatus sits in between the Glomerulus and Distal Convoluted Tubule (where it wraps back around to glomerulus) detecting filtrate rate and quality.
RENIN/ANGIOTENSIN II GIVES THE KIDNEY DIVERSE SYSTEMIC, NEURAL, AND RENAL METHODS FOR MAINTAINING BLOOD PRESSURE DURING STRESS! Low Blood Pressure is a stimulus for the JG Cells to secrete renin into the blood. • Angiotensinogen (made by liver in in-active state) ↓Renin (kidney) • Angiotensin I (found in blood an has low activity) ↓ACE (lung) • Angiotensin II (VERY POTENT HORMONE IN BLOOD!) +Thirst center of hypothalmus-in CNS fluids +Adrenal Cortex secretes Aldosterone to increase Na+ and H2O reabsorption, and potential H+ secretion +Vasoconstriction in kidney and body These Three Will Absolutely Increase Blood Pressure! WHAT HAPPENS IF IT DOES NOT increase B.P? Blood Pressure medication often includes ACE-inhibitors to prevent excess angiotensin II formation in the lung.
How does the body prevent the actions of renin, angiotensin II, vasopressin, and aldosterone from going too far? Why don’t we die of hypertension/salty blood/hypervolemia? • 1) Body only produces hormones when they are needed • 2) Hormones are given a short half-life • 3) Pathway leading to production is regulated • 4) Sometimes regulatory pathways do indeed FAIL! • When they fail hypertension may develop!
During hypertension the heart can become over-stretched resulting in reduced contractility, stroke volume and output. When the atria of the heart are over stretched they produce a hormone called Atrial Natiuretic Factor (or Atrial Natiuretic Peptide) to protect the ventricle. • 1) ANF directly limits NaCl reabsorption in collecting duct. • 2) ANF reduces Na+ reabsorption in the nephron by inhibiting aldosterone release from adrenal cortex. • 3) ANF reduces ADH release from posterior pituitary and prevents aquaporin from working in collecting duct. 1+2+3 mean that less water is kept in the blood. If the volume of blood is decreased then the blood pressure “should” be decreased to levels that are “safe” for the heart. • How do transplanted hearts regulate fluid volume in the recipient? • You thought you were dead, but your heart can still “think”.
TOO MUCH PLASMA • The appropriate response of the body is to decrease the plasma volume. • Stretch of the atria increases ANP • The kidneys increase urine output through loss of Na+ and water