Download
1 / 43
440 likes | 609 Views
New generation anticoagulants Dr Lee Banting 2PHA406 Drug Design. Timeline - the first generations – 1920-1960. 1935 : First clinical trials of heparin (Disc. 1916). 1920s : Sweet clover discovery.

E N D
New generation anticoagulantsDr Lee Banting2PHA406 Drug Design
Timeline - the first generations – 1920-1960 1935 : First clinical trials of heparin (Disc. 1916) 1920s : Sweet clover discovery 1950s : Warfarin synthesized as less potent analogue and first used as rodenticide then used as a human anti-coagulant 1920 1940 1950 1960 1940s : Dicoumarol responsible. A Vitamin K ‘antagonist’ 1960s : First clinical trials of warfarin
Timeline - the next generation – 1980-2011 Late 1980s : fXa identified and validated as a new target using inhibitor Mexican leech antistasin 2004 : Ximelagatran first oral Thrombin inhibitor 2008 : Dabigatran and rivaroxaban approved for short-term VTE 2011 : Apixaban approved for short-term VTE 1980 1990 2000 2011 2006 : Ximelagatran withdrawn due to liver toxicity 1989 : Thrombin (fIIa) crystal structure determined
Coagulation – tissue, cellular mechanisms Click on picture or go to http://www.hopkinsmedicine.org/hematology/Coagulation.swf
Anticoagulation – context; conditions requiring anticoagulation therapy Venous thromboembolism(VTE) – general: medical: familial Atrialfibrilation(AF)– hypertension: CHD: Lung disease: excessive alcohol + Acute coronary syndromes (ACS) – involving the coronary arteries: ST elevation myocardial infarction (STEMI) : non-ST elevation myocardial infarction (NSTEMI) : unstable angina Prosthetic heart valves - valve thrombosis Heparin induced thrombocytopenia – immune mediate paradoxical thrombosis risk Pregnancy – induced hypercoaguability predisposes women to DVT and PE Pediatrics – central venous catheter ; cancer (leukemia); trauma, congenital heart disease
Anticoagulation – therapeutic uses, DPS Ref: Rang & Dale's Pharmacology, 7th Edition pages within Haemostasis and Thrombosis and BNF,62, 140 (2011) and
Current anticoagulation – shortfalls, a need for new agents Current agents – Requiresupervised injections (Heparin) Require blood monitoring to control – efficacy by dose adjustment : drug-drug interactions : inter-patient variability (genetic polymorphisms particularly with warfarin): unpredictable pharmacokinetics and dynamics (Heparin and warfarin metabolized (warfarin by CYPs 2C9, 1A2 and 3A4) both factors are trained medical staff intensive Both demonstrate toxicity (narrow therapeutic window) and have limiting contra-indications
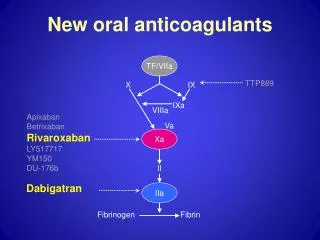
Coagulation cascade – pathways, targets for intervention and sites of drug action Adapted from : http://www.nature.com/nrd/posters/warfarin
Coagulation cascade – yellow / red detailed areas pathway (schematic) Adapted from : Rang & Dale's Pharmacology, 7th Edition pages within Haemostasis and Thrombosis
Thrombin inactivation – molecular detail, thrombin (fIIa), AT III and heparin Green – Thrombin (fIIa) Red – AT III Yellow - Heparin Blue – site of direct inhibition
Factor Xa inactivation – molecular detail, fXa , AT III and LMWH Red – fXa Yellow – AT III Blue – site of direct inhibition Green - The anticoagulant effect of short heparin chains, including the minimal AT-specific pentasaccharide (a LMWH), is mediated exclusively through the allosteric activation of AT towards efficient inhibition of coagulation factor fXa
The targets – what are they? Red – fXa Green – Thrombin, fIIa They are very closely related "trypsin-like" serine proteases with Ser, His and Asp residues as the catalytic “triad” in the active site. Note : Think oral drugs, think trypsin Red/Green overlap
Protein processing by Thrombin and fXa Arginine The S sites are the corresponding enzyme ‘sub-sites’ S2 S1 P2 P1 P1’ P2’ NH2- terminal COOH- terminal S1’ S2’ The P sites are peptide (substrate) residues as numbered from the sissile bond. Thrombin preferentially recognizes Leu-Val-Pro-Arg-Gly-SerFxa tends to like Ile-Glu-Gly-Arg-
Protein C Inhibitor as an active site thrombin inhibitor Thrombin, fIIa (green) PCI Arg (Dark blue, identified as the an active site residue)
Antistasin as an active site fXa inhibitor Arg 32 (green a second Arg nearby) Arg 34 (Blue, identified as the P1 residue) Yellow ring is a double disulphide bond constrained region of the protein
Haemadin as an ‘exosite’ thrombin inhibitor Haemadipsasylvestris(a land-living leech ) Thrombin (yellow) HaemadinArg 21 (Blue, identified as the an ‘exosite’ residue) Haemadin (green)
Target rationale The important functions of thrombin and fXa in coagulation make them choice targets in the search for anticoagulants. Rationales to target either thrombin or fXa have been discussed over the years inhibition of thrombin stops the propagation and amplification of coagulation by preventing the formation of fibrin and thrombin-mediated activation of factors V, VIII, XI, XIII, and platelets and consequently halts further thrombin generation and inhibition of fXa prevents the activation of prothrombin to thrombin and in turn prevents the burst of thrombin without affecting the existing level of thrombin. The residual level of thrombin should be able to ensure primary haemostasis and reduce bleeding risk. As fXa is situated at the junction of the intrinsic and extrinsic pathway and collectively controls the generation of thrombin, it is more effective to target fXa than individual coagulation proteases upstream in the cascade. fXa inhibitors exert their anti-coagulative effect through the control of thrombin generation; therefore, less inhibitory activity should be required. As a result, a fXa inhibitor should theoretically have a wider therapeutic window. Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
Drug development - fXa and thrombin Advances in high throughput screening (HTS) availabilities of crystal structures (1990’s first fXa / drug complexes crystallized) active site knowledge and structure-based design have made both fXa and thrombin attractive and popular targets for drug discovery programs. The development of direct fXa and thrombin inhibitors have been carried out in parallel for the past 20 years. Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
fXa active site - knowledge Disulphide box – hydrophobic region Active site triad Ser S1 pocket – contains an Asp that interacts with the substrate Arg residue His Asp Conserved Gly amide bonds to the P3 of the substrate Cation hole – carbonyl oxygens from these residues like cations S4 / Aromatic Box – hydrophobic region Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
fXa active site - detail As serine proteases, thrombin and fXa share similar secondary structure and protease domains. As seen earlier both of them prefer arginine-like residues at P1 of the substrate (or inhibitors) in order to interact with Asp189 at the base of the S1 pocket. In fXa, a hydrophobic‘‘disulfide pocket’’ adjacent to S1 is formed by Gln192, Cys191, Cys220, and Gly218. The S2 pocket of fXa is obstructed by the Tyr99 side chain and is restricted to small residues such as glycine at this location. A key water exists here too. (In contrast, the S2 site of thrombin contains a prominent hydrophobic pocket created by Trp60D, Tyr60A, His57, Trp215, and Leu99. In addition The “60-insertion loop” (terminology relative to ‘normal serine proteases’) Tyr60A-Pro60B-Pro60C-Trp60D, forms a hydrophobic lid to the S2 pocket in thrombin and discriminates against larger P2 residues.) The amide group of the highly conserved Gly216 provides hydrogen-bonding interactions with the P3 residue of the substrate. In fXa, a characteristic U-shaped aromatic box is formed by Tyr99, Trp215, and Phe174 and also serves as S4. Although a similar hydrophobic region is also found in thrombin, it is formed by the nonaromatic residues Asn98, Leu99, Ile174, and Trp215. This can be used for selective fXa inhibitors. Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
fXa active site - comparisons Also in fXa, the carbonyl groups of Lys96, Glu97, and Thr98 juxtapose to form an electronegative cavity, as known as a cation hole, at the back of the aromatic box. The characteristic U-shaped aromatic box in S4 can be used to design selective fXa inhibitors. Most fXa inhibitors, however, bind to the active site in a characteristic L-shaped conformation The presence of the ‘‘60-insertion loop’’ in thrombin forces inhibitors to adopt a more folded orientation to bury into the enzyme and facilitates the design of thrombin selective inhibitors. Despite the fact that fXa shares much similarity with other serine proteases, such as thrombin and trypsin, enough structural differences exist between fXa, thrombin, and trypsin to provide a structural basis to design selective inhibitors for fXa. Modified from : Lee etal, Med.Res.Rev.,31(2),202-283 (2011) and Bhuniaetal J.Chem.Inf.Model.,51,1966 (2011)
Evolution of fXa inhibitors Amidine forms a “salt bridge” with the Asp in S1 • Phase2 • Asymmetric • Improved selectivity • Poor bioavailability Lower activity against fXa in many cases Higher lipophilicity hence higher plasma protein binding Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
Early fXa inhibitors (b) Mono Weak non-selective 10’s of mM Little more selective 100-1000’s nM Dibasic Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
Dibasic early fXa inhibitors 1,4 - x10 ⬆ x10 ⬇ 1,3 - Cycloheptanone derivatives Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
Amidinesvs non-amidines The X-ray crystallographic experiments have well proven that most amidines form a direct salt-bridge with the Asp residue located in the S1 pocket, whereas nonamidines exhibit indirect chloro-binding mode with a Trp (Tryptophan) located beneath the Asp in the same pocket of both fXa and thrombin. These important residues are completely conserved in fXa, thrombin, and trypsin. The failure of the amidine class of inhibitors to attain a suitable PK profile in terms of oral absorption has served the reason behind the incorporation of neutral P1 motifs (in nonamidines) at this site in order to develop ideal anticoagulants as potential antithrombotic agents. Therefore, current research effort has shifted toward the discovery and development of nonamidine class of selective inhibitors bearing suitable PK profile and robust anticoagulant potential. Modified from : Lee and Player, Med.Res.Rev.,31(2),202-283 (2011)
From first screening -> hit -> lead When Bayer initiated their fXaprogramme (1998) no orally active fXa inhibitors with sufficient antithrombotic activity were known. All known potent inhibitors that had previously been investigated contained an amidine group (or other highly basic residues) that were designed to act as mimics for an arginine present in the natural substrate, pro-thrombin. The mimics were thought to be a prerequisite for high binding affinity. However it was found that these strongly basic mimics contribute to poor oral absorption. Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
HT- Screening to find a hit Bayer high-throughput screened ca. 200,000 compounds finding several hits that selectively inhibited the cleavage of a chromogenic(colour generating) substrate by human fXa. The most potent of these hits was on a minor impurity (serendipity) in a combinatorial library — a phosphonium salt with an IC50 of 70 nM (see Hit). It was suggested that this positively charged phosphonium moiety might be acting as an arginine mimic and could be interchangeable with an amidine group. Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Synthesis and development of a Lead The hit resulted in the synthesis of a lead (see lead) with similar potency IC50 of 120 nM). Optimization resulted in the synthesis of compounds of the isoindolinone class, among which an imidazoline was the most potent (IC50 of 2 nM). In order to achieve oral bioavailability, Bayer explored less basic or non-basic amidine replacements. Aminopyridines, showed IC50 values in the low nanomolar range although they were less basic, oral absorption remained insufficient. A less potent pyridylpiperazine derivative had an IC50 of 48 nM but achieved an improved oral bioavailability of 38% in rats. Although they had demonstrated that improved oral bioavailability could be achieved using less basic amidine replacements, they were not able to meet their target of identifying factor Xa inhibitors with both high potency and sufficient oral bioavailability in the isoindolinone class of compounds. Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Scaffold hopping However, from this approach Bayer learnt that broad variations in the benzylamidine part were permissible, but found from a structure–activity relationship (SAR) of analogues that the chlorothiophenecarboxamide moiety, which was already present in the lead structure was very important. Failure to find a compound with sufficient potency and bioavailability could have ended their project. However, they decided instead to re-evaluate the weaker screening hits. An oxazolidinone from this re-evaluation indicated weak fXa inhibition, with an IC50 of 20,000 nM. Considering the importance of the chlorothiophene residue in the previously studied class of compounds they replaced the thiophene moiety of this compound with a 5-chlorothiophene group, thereby creating an new lead compound which yielded a >200-fold higher potency (IC50 of 90 nM) and did not include a basic group. Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Synthesis and development of the oxazolidinones On the basis of this promising lead, a medicinal chemistry programme was followed that concentrated on increasing the potency of the oxazolidinone class without compromising its pharmacokinetic profile. The starting point of these investigations was the thiomorpholine group; morpholine and pyrrolidine derivatives showed some improvement in potency (IC50 = 32 nM and 40 nM, respectively). Although not sufficiently potent, the morpholine was the first compound to show a favourable PK profile, with a high oral bioavailability of 94% in rats. An ortho-substitution led to the pyrrolidinone, with had significantly improved potency (IC50=4 nM) and an oral bioavailability of 65%. However, the in vivo antithrombotic potency of this compound, evaluated in rats, was estimated to be too low. Bayer’s SAR knowledge then led them to substitute a morpholinone resulting in rivaroxaban, for which binding to factor Xa depends on the (S)-configuration at the oxazolidinone core. Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Drug development of Rivaroxaban (a) IC50=120nM IC50=2nM Oral bioavailability <1% IC50=8nM Oral bioavailability <1% Hit IC50=70nM Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Drug development of Rivaroxaban (b) IC50=48nM Oral bioavailability: 38% IC50=20,000nM, R=H IC50=90nM, R=Cl Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Drug development of Rivaroxaban (c) IC50=32nM Oral bioavailability: 94% IC50=4nM Oral bioavailability: 65% IC50=0.7nM Oral bioavailability: 60% Rivaroxaban IC50=40nM Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Rivaroxaban “comes home” S1 S3 S4 BAY 59-7939 in active site BAY 59-7939 in fXa Modified from : Perzbornetal, Nature Reviews-Drug Discovery, 10,61(2011)
Comparison of Apixaban and Rivaroxaban Red – Apixaban (Pfizer/BMS) Blue - Rivaroxaban (Bayer/J&J)
Where are the fXa inhibitors now - NICE? Atrial fibrillation (stroke prevention) – rivaroxaban http://guidance.nice.org.uk/TA/Wave24/18 Venous thromboembolism (prevention) – rivaroxaban http://guidance.nice.org.uk/TA/Wave26/3 Venous thromboembolism - apixaban (acute medical illness) http://guidance.nice.org.uk/TA/Wave21/18 Venous thromboembolism - apixaban (hip and knee surgery) http://guidance.nice.org.uk/TA/Wave21/17 Eur Heart J. 2011, 32(16), 1968-76, Novel oral anticoagulants: focus on stroke prevention and treatment of venous thrombo-embolism. Steffel J, Braunwald E.
Where are the fXa inhibitors going? “Data from recent large-scale Phase III trials add to the growing evidence that VKAs will most likely be replaced by several novel anticoagulants which will improve substantially the management of stroke prevention in AF, VTE prophylaxis and treatment, and possibly ACS. Awareness of the potential limitations of these drugs as well as continuing research is indispensible for identifying the characteristics of patients who should receive these agents, and the relative advantages and disadvantages of each. ...” Eur Heart J. 2011, 32(16), 1968-76, Novel oral anticoagulants: focus on stroke prevention and treatment of venous thrombo-embolism. Steffel J, Braunwald E.
Have we ‘ideal’ anticoagulants now? Proven efficacy ✓ Low bleeding risk ✓ Fixed dosing ✓ Good oral bioavailability ✓ No routine monitoring ✓ Reversibility ✓ Rapid onset of action ✓ Little interaction with drugs or food ✓ Antidote available ✓ Eur Heart J. 2011, 32(16), 1968-76, Novel oral anticoagulants: focus on stroke prevention and treatment of venous thrombo-embolism. Steffel J, Braunwald E.