Download
1 / 46
480 likes | 593 Views
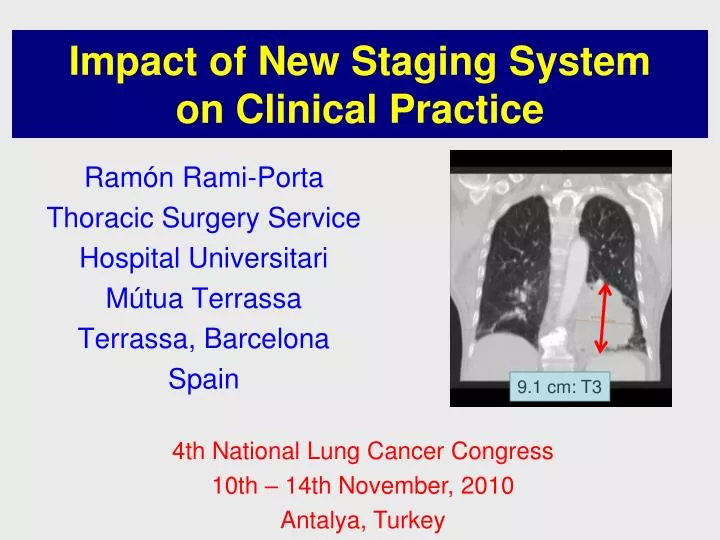
Impact of New Staging System on Clinical Practice. Ramón Rami-Porta Thoracic Surgery Service Hospital Universitari Mútua Terrassa Terrassa, Barcelona Spain. 9.1 cm: T3. 4th National Lung Cancer Congress 10th – 14th November, 2010 Antalya, Turkey. Changes in the 7th edition.

E N D
Impact of New Staging System on Clinical Practice Ramón Rami-Porta Thoracic Surgery Service Hospital Universitari Mútua Terrassa Terrassa, Barcelona Spain 9.1 cm: T3 4th National Lung Cancer Congress 10th – 14th November, 2010 Antalya, Turkey
Axial size 13 mm
Coronal size 22 mm
Axial size T3 8 cm
Axial sizemodifiedby PET scan 4 cm T2b
T Overall survival by tumour size for patients with cT1-T3 N0, UICC 6 classification
T Overall survival by tumour size for patients with cT1-T3 N0, UICC 6 classification 6% absolute difference
Overall survival: cT3 vs same-lobe nodule vs pleural dissemination vs other cT4 factors vs cM1. UICC 6 classification T
Overall survival: cT3 vs same-lobe nodule vs pleural dissemination vs other cT4 factors vs cM1. UICC 6 classification T T3 T4
Survival by number of zones N 1 pN1 zone Several pN1 zones 1 pN2 zone Several pN2 zones
VAMLA Mr. Holger, Dr. Hürtgen, Dr. Witte. Hospital Universitari Mutua Terrassa, 2006
TEMLA Pulmonary Hospital, Zakopane, Poland, 2006. Surgeon: Dr. Marcin Zielinski.
Supermediastinoscopies: Transcervical mediastinal LN dissection
The IASLC lymph node map Rusch V et al. J Thorac Oncol 2009; 4: 568-577
The IASLC lymph node map New supraclavicular zone: N3
The IASLC lymph node map New supraclavicular zone: N3 Enlargement of the subcarinal station
The IASLC lymph node map Fewer patients with N1 and N3 tumours; more patients with N2 tumours for induction therapy and possible resection Enlargement of the subcarinal station
The IASLC lymph node map Shift of the anatomic midline to the left paratracheal border
N2 for right-lung cancer N3 for left-lung cancer
Inclusion of more patients with N2 disease in induction protocols; and more patients to assess for resection after induction N2 for right-lung cancer N3 for left-lung cancer
The IASLC lymph node map Some #10 LNs (hilar LNs) are in the mediastinum
Global survival: best staging M Resection of synchronous bilateral lung cancer 5-year survival: 38% De Leyn P et al. Eur J Cardiothorac Surg 2008; 34: 1215-1222
Stage grouping Adjuvant chemotherapy?
Stage grouping Adjuvant chemotherapy? Primary resection for selected cases and surgeons? Induction and resection?
NSCLC: Clinical Impact • Prognosis: • size matters: precise measurement and careful watch of SPNs! • contralateral nodules may be second primaries • Staging: • some TNM subsets shift stage • more thorough evaluation of nodal extension to identify involved nodal zones • Treatment:a change of stage does not mean change of treatment. Clinical judgement and best evidence, in the abscence of RCTs, will guide therapeutic decisions
Overall survival for clinical TNM stage categories SCLC, IASLC database Limited disease IASLC 1989
% of agreement between c and p Vallières E et al. JTO 2009; 4: 1049-59
Survival of resected SCLC by 6th edition Vallières E et al. JTO 2009; 4: 1049-59
Survival of resected SCLC by 6th edition Vallières E et al. JTO 2009; 4: 1049-59
Survival of pN by pT1-4 M0 Vallières E et al. JTO 2009; 4: 1049-59
Survival by p stage: 6th and 7th editions p HR Vallières E et al. JTO 2009; 4: 1049-59
Survival by p stage: 6th edition Shepherd FA et al. JTO 2007; 2: 1067-77 Vallières E et al. JTO 2009; 4: 1049-59
Survival by p stage: 6th edition Completely resected SCLC. Lim E. JTO 2008; 3: 1267-1271 60% 50% Shepherd FA et al. JTO 2007; 2: 1067-77 Vallières E et al. JTO 2009; 4: 1049-59
Small cell lung cancer: Stage grouping 38% 21% 38% 18% 13% 9%
SCLC: Clinical Impact • Prognosis: TNM classification prognosticates better than the traditional dichotomous classification • Staging: TNM classification implies a more intensive evaluation of tumour extent • Treatment: TNM classification may identify some tumours for resection or smaller radiotherapy field. RCTs, needed
Conclusions • for both NSCLC and SCLC, the 7th edition of the TNM classification improves our capacity to assign a prognosis to a certain tumour • the use of the TNM classification for SCLC may need a more thorough clinical evaluation • TNM subsets that are stage shifters may raise doubts about their best treatment options