Download
1 / 56
560 likes | 665 Views
Current Issues in the Management & Prevention of Sexually Transmitted Diseases. John M. Douglas, Jr., MD Denver Public Health. Estimated Burden of STD in U.S. --1996. STDs: Why Should We Care?. 1. PID and infertility 2. Adverse outcomes of pregnancy 3. Cancer

E N D
Current Issues in the Management & Prevention of Sexually Transmitted Diseases John M. Douglas, Jr., MD Denver Public Health
STDs: Why Should We Care? 1. PID and infertility 2. Adverse outcomes of pregnancy 3. Cancer 4. Acquired immunodeficiency syndrome 5. Enhanced HIV transmission
STD/HIV among MSMin the HAART Era • Dramatic increase in STD in gay men, especially in western US • increase in GC, 25% of whom are HIV+ • outbreaks of syphilis in Seattle, SF, LA, 25-75% HIV+ • recent 3-fold increase in HIV incidence in SF (1.3%-3.7%) • Increases in risk behaviors • HAART-associated return to health among HIV+ • HAART “optimism” among both HIV+ & HIV- • Prevention burn-out • Internet access to anonymous partners • Among HIV+, increased risk behaviors may be accompanied by poor HAART adherence: • Increased likelihood of HIV transmission • Emergence of drug-resistant strains
Emerging Issues in STD 1. New STD diagnostic approaches 2. Updated (2002) CDC STD Treatment Guidelines 3. Interaction of the STD and HIV epidemics
Nucleic Acid Amplification Tests (NAATS) for GC/CT • Current options: • PCR (polymerase chain reaction, Amplicor) • LCR (ligase chain reaction, LCx) • SDA (strand displacement assay, ProbeTec ET) • TMA (transcription mediated amplification, Amp CT) • Can be used to detect GC/CT in same specimen; limited data on rectal or pharyngeal specimens • Single day turnaround, but cost is an issue ($12->$50 per test) • 90-95% sensitive, 98-99% specific (though some concerns about FP and FN, especially with GC) • Extreme sensitivity allows “non-invasive” sampling of urine (also tampons, vaginal secretions)
Screening for CT • All sexually active women < 25 annually • Sexually active adolescents 4-6 months post-RX of prior CT infection • Other women (women > 24 or < 25 with CT- test in past year) if: • evidence of other newly acquired STD • multiple partners, new partner (especially if young), or partner with multiple partners • symptoms/signs of CT • Pregnant women: first prenatal visit; re-screen at-risk F in 3rd trimester to prevent maternal postnatal complications/infant transmission • Men: • Heterosexual: no evidence to support screening--issue is whether cost-effective; consider adolescent M if urine-based NAAT available • MSM: annually (urethral and rectal), more frequently if high-risk
Screening for GC • Women • no guidelines yet due to marked geographic variability in GC prevalence (variation by region, ethnicity, SES) • in absence of local data, reasonable to consider as for CT, although beware of potential false positives • pregnancy: first prenatal visit & 3rd trimester if “at risk” or high prevalence population • Men • heterosexual men--no guidelines; urethral screening likely to be low yield given high attack rate if infected. • MSM--recent guidelines recommend annual screening (urethral, rectal, pharyngeal), more frequently if multiple partners or drug use
Antimicrobial Resistance of GC/CT • GC resistance is widespread • 20-30% of US strains resistant to either PCN or TCN: 8-10% PPNG; 10-20% CMRNG for PCN, TCN; 3-5% TRNG • Limited resistance to 3rd generation cephalosporins, but emerging quinolone resistance, especially in SE Asia, now also Hawaii & CA • CT resistance to TCN reported in isolated cases, but extremely limited
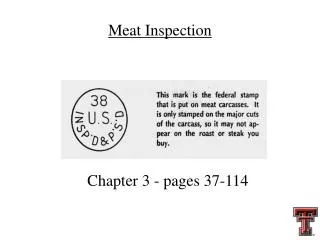
Gonococcal Isolate Surveillance Project (GISP) — Percent of Neisseria gonorrhoeae isolates with decreased susceptibility or resistance to ciprofloxacin, 1990–2000 Note: Resistant isolates have ciprofloxacin MICs >1 mg/mL. Isolates with decreased susceptibility have ciprofloxacin MICs of 0.125 - 0.5 mg/mL. There were sixty-one (61) resistant isolates: one in 1991, one in 1993, two in 1994, eight in 1995, two in 1996, five in 1997, four in 1998, nineteen in 1999, and nineteen in 2000. Susceptibility to ciprofloxacin was first measured in GISP in 1990.
Gonorrhea--RX Issues • Quinolones should not be used for infections acquired in Asia/Pacific/Hawaii/California • Presumptive co-RX for CT (recommended since 1985) • is cost effective if co-infection rate 10-30% because cost of testing exceeds cost of RX • if CT infection is ruled out by using a highly sensitive CT test (NAATs), then co-RX not needed • can consider testing rather than treating if local co-infection is low, a sensitive test is used and patient is likely to return for test result • be aware of potential problems with N/V after co-treatment using azithromycin, especially on empty stomach--may need to offer pre-RX food with directly observed therapy
Chlamydial InfectionTreatment in Adolescents and Adults Recommended regimens: • Azithromycin 1 g PO x 1 or • Doxycycline 100 mg PO BID x 7 d Alternative regimens: • Erythromycin base 500 mg PO QID x 7 d * or • Erythro ethylsuccinate 800 mg PO QID x 7 d * or • Ofloxacin 300 mg PO BID x 7 d or • Levofloxacin 500 mg PO QD x 7 d
ChlamydialInfection Treatment in Pregnancy • Recommended regimens: • Erythromycin base 500 mg PO QID x 7 d or • Amoxicillin 500 mg PO TID x 7 d • Alternative regimens: • Erythromycin base 250 mg PO QID x 14 d or • Erythro ethylsuccinate 800 mg PO QID x 7 d or • Erythro ethylsuccinate 400 mg PO QID x 14 d • Azithromycin 1 g PO x 1( “clinical experience of some experts and preliminary data suggest that azithromycin is safe and effective”) • Test of cure in 3-4 weeks
Recommended RX for GC • Anogenital infection • ciprofloxacin 500 mg PO X 1 • ofloxacin 400 mg PO X 1 • levofloxacin 250 mg PO X 1 • ceftriaxone 125 mg IM X 1 • cefixime 400 mg PO X 1--NOT AVAILABLE (other options: cefuroxime axetil 1 g PO, cefpodoxime proxetil 200 mg PO) • PLUS RX for chlamydia • B-lactam allergy: quinolone or spectinomycin 2 g IM X 1 • Pregnancy: cephalosporin or spectinomycin • Pharyngeal: ceftriaxone or ciprofloxacin (not ofloxacin/levofloxacin) • Conjuncitivitis: ceftriaxone 1 g IM X 1
Partner-delivered Therapy for CT & GC • Inability to successfully treat partners (usually male) associated with high rates of re-infection • Partner-delivered therapy found to reduce re-infection rate by 20% (Schillinger et al) • A potential legal issue in some states, but in Colorado considered appropriate by State Board of Medical Examiners (“...the public risk of untreated STD is greater than the risk of complications from prescribing in this less than ideal setting.”, policy 40-10, 5/10/01)
Genital Ulcer Disease • Syphilis (T. pallidum) • Genital herpes (HSV-2,-1) • Chancroid (H. ducreyii) • Lymphogranuloma venereum (C. trachomatis) • Granuloma inguinale
Syphilis elimination in the U.S. • National Plan to Eliminate Syphilis launched 10/99 • Definition: absence of sustained transmission (no transmission > 90 days after report of index case) • Operational goals: reduce primary & secondary syphilis to < 1000/yr (0.4/100,000) • Recent trends of P/S (compared to 6500 in mid-50s, >50,000 in 1990) : • 1997--8556 cases • 1998--7035 cases • 1999--6657 cases • 2000--5894 cases • 2001--6103 cases • 2002--6551 cases (provisional total) • 2001-2: 19% increase in M, 26% decrease in F
Syphilis in Denver by Stage and Sexual Orientation 2001 and 2002
Primary Syphilis • Painless papule at inoculation site progressing to ulcer (chancre); most often detected in heterosexual men. • Incubation 7-90 days (most 14-21) depending on inoculum size • Typical chancre: 0.5-1.5 cm, painless, clear base and indurated border, with bilateral nontender LN • Atypical lesions: > 50%, multiple lesions (25%), superinfected with bacteria or other GUD • Prior infection “modifies” (papule, not ulcer; DF neg) • DX: darkfield(?80% sensitive, most specific); RPR(80% sensitive); FTA (90% sensitive and earlier)
Secondary Syphilis • Myriad symptoms as result of hematogenous dissemination • Generally appears 30-70 days after chancre (35-160 days after exposure); chancre still present in 15% • Skin rash most common finding: usually mild evanescent macular rash-->symmetric papular lesions (scaly, follicular, pustular, papulosquamous; rarely vesicular; often palms/soles) • Less common mucocutaneous findings: condyloma lata (anogenital, also mouth, face, axilla) , mucous patches, alopecia
Diagnosis of Syphilis • Essentially no new approaches; keys to diagnosis are • Darkfield exam or DFA of lesion exudate or tissue are definitive methods (early syphilis) • Presumptive diagnosis with nontreponemal tests (VDRL,RPR) and treponemal tests (FTA-ABS,TP-PA); use of only one serologic test is insufficient for diagnosis • Nontreponemal tests usually correlate with disease activity, while treponemal tests usually persistently reactive
Treatment of Syphilis • Early (primary, secondary, early latent): • benzathine PCN 2.4 mu IM X 1 dose • NEW: ceftriaxone 1 g IM qd X 8-10 days; azitrhromycin 2 g X 1--limited data!! • Late latent (> 1 yr. duration) • benzathine PCN 2.4 mu IM X 3 doses • if PCN-allergic: doxycycline X 4 wks; no data on ceftriaxone and azithromycin • Neurosyphilis: • PCN G IV or IM qd X 10-14 days; ceftriaxone 2 g IV/IM X 10-14 days • Pregnancy or HIV+ • use PCN in all; desensitize if allergic
Diagnosis of Neurosyphlis • Criteria for CSF exam • Neurologic or ophthalmic symptoms/signs • Evidence of tertiary disease (aortitis, gumma, iritis) • RX failure (failure of titers to decline 4X in 6 mos for early syphilis and in 12-24 mos for late syphilis) • HIV+ with late latent or unknown duration • Some experts recommend a CSF exam in all patients with latent syphilis and a titer 1:32 • Diagnostic criteria • Ocular disease (uveitis, retinitis) with reactive STS • Abnormal CSF (+RPR--70%, increased WBC, increased protein) in absence of another explanation
Syphilis: Follow-up after Treatment • Partners at risk: 3 m + sx for primary, 6 m + sx for secondary, 12 m for early latent or latent of unknown duration • Patient serologic follow-up: • for primary/secondary, re-test 6 and 12 m; re-RX if symptoms/signs or 4X titer RPR increase • for latent, re-test 6,12, 24 m; LP and re-RX appropriately if symptoms/signs, 4X titer increase, initially “high” titer (> 1:32 fails to fall 4X)
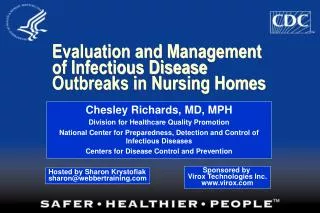
Genital herpes simplex virus type 2 infections — Percent seroprevalence according to age in NHANES II (1976–1980) and NHANES III (1988–1994) Note: Bars indicate 95% confidence intervals. *National Health and Nutrition Examination Survey
Genital Herpes: Diagnosis • Overview: • Clinical DX can be both insensitive/nonspecific, and because of lifelong implications, lab confirmation important • Helpful to have both virologic & serologic tests in settings caring for patients with STD • Virologic DX: • culture--preferred test, but sensitivity falls as lesions heal • antigen--more widely available; some don’t distinguish HSV-1 and -2 • PCR--limited availability; evaluated for CSF but not lesions
Genital Herpes: Serologic Tests • Several newly licensed type-specific tests based on Aby to glycoprotein G • HSV-2 specific for anogenital infection, HSV-1 can be anogenital or oral • Available as EIA (HerpeSelect EIA) & immunoblot (for HSV-1 and -2) and point-of-care test ( POCkit HSV-2) • Sensitivities 80-98%; specificities > 96%. Consider repeat test or a 2nd test (immunoblot) if low probability of infection • Non gG-based assays are still on market, less accurate • Potential uses: culture-negative ulcers with recurrent lesions, partners; not yet for general screening
Screening for HSV-2? • Serologic screening beyond those with lesions or partners not recommended • some experts believe it can be useful in pregnant women to identify those at risk of acquiring infection (also involves partner testing), though concerns over increased use of C-sections • wider screening (eg, STD clinics) theoretically useful in identifying those with asymptomatic infection who could then recognize outbreaks and prevent transmission
Treatment of Genital Herpes • First episode (10 days recommended) • acyclovir 200 mg 5 X/day or 400 mg PO tid (est. $40-50) • valacyclovir 1 g bid (est. $100-120) • famciclovir 250 mg tid (est. $95-120) • Recurrent episode (5 days recommended) • acyclovir 200 mg 5 X/day or 400 mg PO tid (est. $20-25) • valacyclovir 500 mg bid of 1 g qd (est. $40-50) • famciclovir 125 mg bid (est. $30-40)
Genital Herpes: Suppressive Treatment • ACV 400 mg bid • FCV 250 mg bid • VCV 500 mg qd • VCV 1 g qd (if very frequent recurrences)
Genital Herpes: Counseling--General Guidelines • Goals: patient coping and disease transmission • HSV-specific resources available and helpful: printed materials, websites (www.ashastd.org), hotlines (800-227-8922) • Key issues to cover: • severity of initial and recurrent episodes • sexual relationships and transmission • obstetrical issues
Genital Herpes: Counseling--Key Messages • Education about natural history (recurrences, asymptomatic shedding) and episodic and suppressive RX • Encouragement to inform current & future partners • Avoid sex with uninfected partners during outbreaks • Asymptomatic shedding (1-5% of days) can transmit infection; more common first yr of infection and for HSV-2 • Condoms used consistently & correctly can reduce risk (from M to F and likely F to M) • Partners of those with herpes can be asymptomatically infected; serologic testing can determine risk of infection • Asx HSV-2+ persons can be taught to recognize outbreaks (60%) and be counseled as for symptomatic
Genital Herpes: Counseling--Key Messages to Prevent Neonatal HSV • Explain risk of neonatal HSV to both M & F • Pregnant women with herpes should inform provider • Pregnant F known not to have HSV-2 should avoid sex in third trimester with M who do • Pregnant F known not to have HSV-1 should avoid sex in third trimester with M who do (eg, cunnilingus if history of oral herpes and genital sex if known history of genital HSV-1)
Condoms for Prevention of Genital HSV Infection • Theoretically less likely to be effective for infection of external genital epithelium than for infections of mucosal surfaces/semen (GC, HIV), although condoms likely cover sites of greatest asymptomatic shedding, especially in men • Several studies suggest benefit in discordant couples (probably asymptomatic shedding transmission) • 144 discordant partners in vaccine study, annual transmission risk 5.7% in condom/diaphragm users vs 13.6% in non-users (Mertz Ann Int Med 1992; 116:197) • 531 discordant couples in vaccine study, condoms provided benefit for women (11.7 HR) but not men (Wald, JAMA 2001)
Genital HPV Infection • Low-risk types (6,11) • genital warts and low-grade Pap smear changes (ASCUS, LSIL) • Higher-risk types (16, 18, 31, 33, 35, others) • LSIL and HSIL • All types cause subclinical infection
Therapy of Genital Warts: Overview • Goal of therapy is elimination of symptoms • Treatment MAY reduce infectivity but will not eradicate infection • Multiple treatments usually required and recurrences common (20-50%)
Treatment of Genital Warts • Patient-applied • Podofilox bid x3, off x4; 4-6 cycles • Imiquimod x3/wk for up to 12-16 weeks • Neither approved for use in pregnancy
Treatment of Genital Warts • Provider-applied (once/weekly) • Cryotherapy* • Podophyllin • Trichloracetic acid* • Office surgery*-excision, electrocautery, curettage *Safe for use in pregnancy
HPV Testing for Triage of Low-grade Pap Smear Abnormalities • Low-grade abnormalities (ASCUS, AGUS, LSIL) present in 5-10% of U.S. Pap smears, and 5-20% have CIN 2/3 on biopsy • Cost of conservative management (colposcopy/biopsy) $ 3-4 billion per year. • Commercial HPV tests have high sensitivity (90%) and specificity similar to FU Pap smear (65%) for ASCUS, but nonspecific with LSIL • Use unlikely to prevent cancer, but could save money; cost-effectiveness analyses will be critical
2001 Consensus Guidelines for Management of Abnormal Cytology* ASC-US HPV testing (if liquid-based cytology) or FU Pap or Colpo ASC-H Colpo + endocervical sampling LSIL Colpo (or in post-menopausal or teens FU Pap smear 6-12 mos or HPV test 12 mo HSIL Colpo (or LEEP if poor FU or older) *Guidelines of Am Soc Colpo & Cervical Path. Wright et al. JAMA 2002; 287:2120
HPV Infection: Counseling • Genital HPV is highly prevalent viral STD • Virtually always sexually transmitted, variable incubation, hard to determine infection source; current partners usually already infected by DX • Natural hx of EGW usually benign; usually not associated with HR types • Wart recurrence common; usually not re-infection • Duration of infectivity after RX& chance of transmission to future partners unknown. Condoms poorly studied; but associated with lower rate of cervical cancer • Because of high prevalence and imprecise natural history, value of disclosure to future partners unclear; though candor between partners encouraged whenever possible
Condoms for Prevention of Genital HPV Infection • Less likely to be effective for infection of skin than for infections of mucosal surfaces/semen (GC, HIV), although studies limited by difficulty in measuring infectivity and incident infection • Studies in women have generally found no evidence of benefit, although haven’t assessed consistency and correctness of use and most are cross-sectional • Limited studies suggest possible benefit in men • Some reports suggest benefit in prevention of HPV-related disease (e.g, GW, SIL, cancer) possibly by reducing viral inoculum, repeated exposure, exposure to other co-factors
Role of STD in Enhancing HIV Transmission: the Evidence • Emerging body of data indicating • enhanced susceptibility due to reduced mucosal barriers and increased target cells • enhance infectivity due to increased HIV in genital lesions, secretions, semen • Evidence largely based on epidemiologic studies, with increased rates of HIV from 3-5 X for mucosal STD and 2-12 X for GUD • Two intervention studies of STD control to prevent HIV in Africa with mixed results: enhanced STD services with 40% reduction in HIV, mass STD RX with no benefit
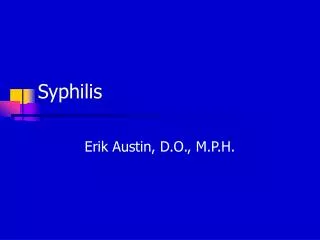
Probability of HIV Transmission in 174 Monogamous Couples: Rakai, Uganda Wawer M, Gray R, Quinn TC, et al Int’l Retrovirus Meeting 2001
STD/HIV Interaction: Implications in the US • National Syphilis Elimination Campaign is targeting reduction in sustained domestic transmission (to < 1000 cases from current 5500/yr) to prevent both perinatal morbidity & enhanced HIV transmission • Re-emerging risk behavior and STD/HIV epidemics in MSM • dramatic increases in STD in MSM past 4 yrs: increase in GC (25% HIV+) and syphilis (25-75% HIV+), recent 3X increase in HIV in SF • new CDC recommendations for STD screening in MSM: annually for HIV, syphilis, GC (urethral, rectal, pharyngeal) and CT (urethral and rectal), more frequently if multiple partners or drugs; no evidence for HSV-2