Download
1 / 34
390 likes | 490 Views
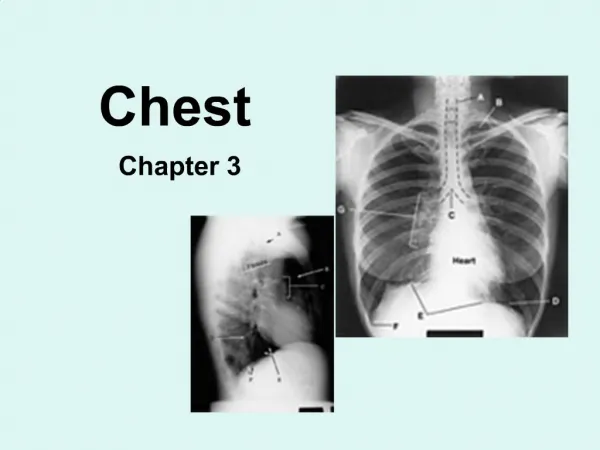
Chest Tubes. Fadi J. Zaben RN NSN. Our lungs are protected by 24 ribs, which also shape and support the chest wall. The parietal pleura is a membrane lining the chest cavity. The visceral pleura is a membrane lining the lungs.

E N D
Chest Tubes Fadi J. Zaben RN NSN
Our lungs are protected by 24 ribs, which also shape and support the chest wall. The parietal pleura is a membrane lining the chest cavity. The visceral pleura is a membrane lining the lungs. The space between these two membranes is known as the intrapleural space. This potential space has a thin film of fluid to provide lubrication and cohesion between the parietal and visceral pleura. Review of Anatomy and physiology
What are chest tubes used for? • Chest tubes are long, clear plastic tubes that are placed in the pleural or the mediastinal space to evacuate an abnormal collection of air or fluid that collects as a result of injury, disease, or surgical procedures. • If the lung has been decompressed because of this collection, the lung can then re-expand.
Indications First: Pneumothorax: a collection of air in the pleural space. • After central line insertion • After chest surgery, • After trauma to the chest, • After a traumatic airway intubations.
If the air continues to collect in the chest, the pressure in that collection can rise and push the whole mediastinum over to the other side – this is called a “tensionpneumothorax”, and is definitely life-threatening.
Second: Hemothorax: A collection of blood in the pleural space, may be from surgery, may be from a traumatic injury. This is actually A hemo-pneumo-thorax: blood and air…
Third: Pus can collect in the pleural space “Empyema”. Fourth: Fluid, usually serous, may be from CHF, sometimes from a tumor process, will collect between the pleura“Pleural Effusion”. To prevent collection of fluid/air. eg : after thoracotomy Post operative; eg cardiac surgery.
Equipment For Insertion: • Several pairs of sterile gloves. • Sterile drape, betadine solution. • Vial of 1% lidocaine. • Alcohol sponge. • 10cc syringe. • 22G 1 inch and 22G 5/8th inch needles. • Sterile forceps and scalpel. • One rubber tipped clamp for each chest tube inserted, sterile gauze pads; sterile 4x4s. • Sturdy elastic tape and scissors. • The chest tube, a trochar, suture kit. • The thoracic drainage system with its collection tubes.
Consist of a trochar is cannula and a long plastic tube about 1.8 m. Many sizes from 8F to 32FG: • Small (24FG): for air alone • Medium (28FG): for serous fluid • Large (32-36FG): for blood/pus • At least 28FG in traumatic pneumothorax to prevent occlusion with blood clot. Smaller size for simple pneumothorax. • Children: size depends on age & distance between the ribs.
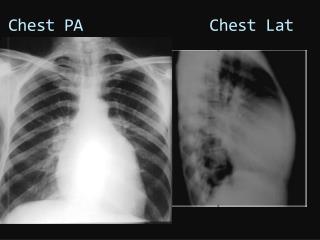
Pre-insertion Documentation Should Include the Following: • Cardiopulmonary assessment (heart and lung sounds). • Heart rhythm if on ECG monitor. • Vital signs. • SpO2. • ABG (if ordered). • Chest x-ray. • Any pain medication or sedative that physician orders prior to and during the procedure. • Your interactions with the physician. • Any patient and or family teaching.
Chest Tube Insertion: • The physician will surgically insert the tube through the chest wall. • It may occur in the emergency room, a hospital room or and operating room depending on patient needs. • The skin is cleaned with antiseptic solutions. • The place the tube is to be inserted is injected with a local anesthetic to numb the area.
Continue……. • Where chest tubes are placed depends on whether fluid or air needs to be drained. • Immediately after placement the chest tubes will be connected to drainage tubing an drainage container. • After placement, the chest tubes are sutured to the chest wall and an airtight dressing is placed over the insertion site.
The chest tube is inserted between the fourth to sixth intercostal space at the midaxillary line to drain hemothorax. The patient will be sat up and leaned over a bedside table.
A person with a pneumothorax will be placed in the supine, high-Fowler’s or semi-Fowler’s position, according to the preference of the person inserting the tubes. • The tube will be inserted into the second or third intercostal space in the anterior chest at the midclavicular line.
Chest Tube Drainage System The first compartment collects fluid and air from the chest cavity The second compartment is sealed with water to keep air from being sucked back into the chest. The third part is used to supply suction to the system
Post-Insertion documentation should include the following: • Date, time, and physician who inserted the chest tube • Description of how the patient tolerated the procedure • Size and location of chest catheter • Completion of post procedure chest x-ray • Cardiopulmonary assessment (post procedure) • Vital signs, including SpO2 • If drainage present, color, amount and type • Any patient and or family teaching
Three primary objectives in caring for the patient with chest tubes are the following: • Keep the system patent. • Maintain sterility of the system to avoid introducing bacteria into the intrapleural space. • Keep the system airtight.
The nurse has the responsibility to maintain an intact and patent pleural drainage system. Check and ensure patency of the chest catheter Check for drainage amount, color, and consistency Check for kinks or dependent loops in tubing, by starting at insertion site and following to drainage system Check water-seal for appropriate level and all connections tight Check to see if water level rises on inspiration and falls on expiration Include the following assessment:
Check for bubbling or fluctuations in the water seal chamber, this will indicate a leak between the patient and the water seal or can indicate that the pneumothorax has not resolved yet If order for gravity drain, Check to see that the suction tubing has been disconnected and open to air Check for chest x-ray order chest tube
Monitor for air leaks, chest x-ray results, oxygen saturations Assess water levels in drainage unit each shift and correct fluid levels if not as ordered • Report to Physician immediately any change or complication with the chest tube.
Complications • Tension pneumothorax • Malpositioned tube • Penetration of peritoneal cavity. • Penetration of heart/major vessels. • Pleural sepsis. • Failure of lung to re-expand.
The most serious complication result from the chest tube placement is tension pneumothorax, which develop if there is any obstruction in the chest tube drainge system Clamping chest tubes as a routine practice predisposes patients to this complication Clamping is recommended: To locate the source of an air leak if bubbling occurs in the water seal champer To replace the chest tube drainge unit
Pleural sepsis. - signs : pt febrile, drain site inflamed, purulent drainage remove drain & start antibiotics - accumulation of pus may need needle aspiration / further drainage thro’ separate site.
Indications for chest tube removal • One day after cessation of air leak • Drainge of less than 50 ml of fluid per day • 1-3 days post cardiac surgery • 2-6 days post thoracic surgery • Obliteration of emphysema cavity • Serosanguineous drainge from around the chest tube insertion site
Nursing diagnosis Impaired gas exchange related to air and fluid collection in lungs and pleural space as manifested by: chest tube, decreased breath sounds, abnormal pulse oximetry Expected patient outcomes Full expansion of lungs Normal breath sounds bilaterally Normal puls oximetry
Nursing interventions • Monitor chest drainage system to ensure a adequate ventilation and to detect hemorrhage • Monitor respiratory rate and pattern and manifestations of hypoxia to allow early recognition of significant changes in respiratory function • Administer low flow oxygen via nasal cannula to treat hypoxemia • Assist with position changes to increase patient comfort and facilitate aeration of the lungs
Risk to infection at the site of chest tube insertion Expected patient outcomes No infection of the wounds absence of signs and symptoms of infection no elevated in the temperature or any laboratory tests.