Download
1 / 13
170 likes | 406 Views
Neonatal Chest Tubes. By: Jodi Tidwell BSN, RN. Definition. To place a tube in the pleural space to decompress a tension pneumothorax or fluid accumulation in order to allow adequate lung expansion for ventilation. Indications for Chest Tube Placement.

E N D
Neonatal Chest Tubes By: Jodi Tidwell BSN, RN
Definition • To place a tube in the pleural space to decompress a tension pneumothorax or fluid accumulation in order to allow adequate lung expansion for ventilation.
Indications for Chest Tube Placement • Pneumothorax - collection of air in the pleural space • Tension pneumothorax – one way valve effect allowing air to enter the pleural space but not leave. Air fills up forcing a mediastinal shift. This leads to decreased venous return to the heart and lungs causing acute life-threatening respiratory and cardiovascular compromise. A tension pneumothorax can result in rapid clinical deterioration and is an emergency situation.
Indications for Chest Tube Placement • Post operatively e.g. cardiac surgery, thoracotomy • Pleural effusion – accumulation of fluid in the pleural space. Four types of fluid can accumulate in the pleural space: • Serous fluid (hydrothorax) • Blood (haemothorax) • Chyle (chylothorax) • Interesting facts: Symptoms of congenital chylothorax are present in approximately 50% of all cases at birth and virtually all cases are diagnosed within the first week of life. Morbidity in neonates born with the disorder ranges from 20-60%. Chylothorax occurs twice as often in male neonates compared with females and is more commonly seen on the right side of the thorax. Congenital chylothorax is more likely in neonates born with Turner’s, Down’s or Noonan’s syndromes. • Pus (pyothorax or empyema)
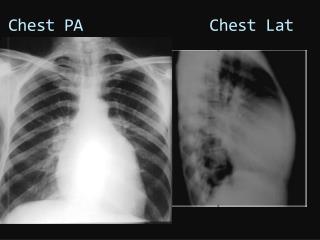
Indications for Chest Tube Placement • X-ray note! If a pneumothorax is suspected, the infant should be lying with the suspected side up during the lateral decubitus x-ray. If a pleural effusion is suspected, the infant should be placed with suspected side down. In this way, layering out of the air or fluid may occur so that a lung margin is seen separated from the chest wall by the air or fluid in the intrapleural space. pneumothorax Pleural Effusion
Materials needed • Pain medication ordered by physician • 1% Lidocaine, 1 ml syringe with 25 gauge needle • ChloraPrep • Sterile gloves, masks, and hat (gown optional) • Sterile tray to include: • 4 x 4’s • 2 x 2’s • Drapes • Curved mosquito hemostats • Scissors • Sterile thoracotomy tube (10 F for infants under 1500 grams and 12 F for infants over 1500 grams) • Scalpel • 4-0 silk suture on cutting needle • Petroleum soaked gauze • Underwater sealed drainage /Dry suction drainage system
Management of Patient and Drain • Pre-treatment evaluation: • Monitor the patients’ cardiorespiratory status and oxygen saturations throughout the procedure. • Premedicate infant for pain control. Chest tubes are painful as the parietal pleura is very sensitive. Assess need for further medication throughout the procedure. • Position the patient supine with the affected side slightly elevated and the arm on the affected side restrained superiorly (over the head) or anteriorly.
Management of Patient and Drain • Assist physician with procedure • Chest Drain Set Up • Perform hand hygiene • Open drain packaging in a clean manner • Prepare drain as per manufacturer’s instructions • Pass sterile end of tubing to physician inserting drain when they are ready • Apply suction to drain if ordered • Secure drain and tubing to bed and patient • Perform hand hygiene
Drains and Tubing • Never lift drain above chest level • The unit and all tubing should be below patient’s chest level to facilitate drainage • Tubing should have no kinks or obstructions that may inhibit drainage • Ensure all connections between chest tubes and drainage unit are tight and secure • Tubing should be anchored to the patients skin to prevent torqueing and pulling the patients skin • In NICU the tubing should also be secured to the patient bed to prevent accidental removal • Ensure the unit is securely positioned
Suction • If suction is required, orders should be written by medical staff Atrium Oasis Dry Suction Water Seal Chest Drain: • Wall suction should be set at >80mmHg or higher • The bellows should be out to the arrow mark @ 20cmH20 • Any visible expansion of the bellows is adequate for suction <20cmH20 • If the bellows deflate, check the wall suction is still working, set to >80mmHg and that the suction tubing is not kinked
Drainage • Milking or Stripping of chest drains is only to be done with written orders from medical staff. Stripping drains creates a high negative pressure that can cause pain, tissue trauma and bleeding and increases the risk of tube removal. • Document volume and color of drainage throughout shift. If there is a change (for example: from haemoserous to bright red or serous to creamy) notify physician. • Observe for signs of infection and inflammation and document findings • Check dressing is clean and intact. If not, notify physician for dressing change orders. • Observe sutures remain intact and secure
Dressings • Dressings should be changed if: • No longer dry and intact, or signs of infection e.g. redness, swelling, exudate • Infected drain sites require daily changing, or when wet or soiled • This procedure is a risk for accidental drain removal so avoid unnecessary dressing changes and always notify physician before changing the dressing.
References Dublin, PJ and Gallagher, PG. (2000). Congenital chylothorax. Current Opinions inPediatrics, 12, 505-509. Rocha, G. (2007). Pleural effusions in the neonate. Current Opinions in Pulmonary Medicine, 13, 3-5. Shreiner, RL. (2009). Chest Tube Insertion in Neonates. Vol. 237. No. 21.