Download
1 / 28
770 likes | 2.91k Views
Chest Tubes. By Diana Blum MSN Metro Community College NURS 2520. OBJECTIVES. DEMONSTRATE THE ROLE OF THE RN IN NURSING INTERVENTIONS OF CHEST TUBES PERFORM THERAPEUTIC NURSING INTEVENTIONS TO CLIENTS WITH CHEST TUBES. Where exactly is a chest tube placed?

E N D
Chest Tubes By Diana Blum MSN Metro Community College NURS 2520
OBJECTIVES • DEMONSTRATE THE ROLE OF THE RN IN NURSING INTERVENTIONS OF CHEST TUBES • PERFORM THERAPEUTIC NURSING INTEVENTIONS TO CLIENTS WITH CHEST TUBES
Where exactly is a chest tube placed? The entry point is the fourth or fifth intercostal space, on the mid-axillary line. The tube is inserted towards the collection: sometimes up and in front, or up and in back, or wherever the collection lies.
EDUCATE ON WHAT A CHEST TUBE IS TO THE CLIENT • ASSURE A CONSENT FOR PLACEMENT WAS OBTAINED • OBTAIN VITAL SIGNS PRIOR TO PROCEDURE • SET UP ROOM WITH CORRECT EQUIPMENT • WET VS DRY SYSTEM
Chest tubes are inserted to drain blood, fluid, or air and allow full expansion of the lungs. placed in the pleural space. The area where the tube will be inserted is numbed PLACE THE CLIENT IN SEMI FOWLER’S TO HIGH FOWLER’S The chest tube is inserted between the ribs into the chest and is connected to a bottle or canister that contains sterile water. Suction is attached to the system to encourage drainage. A stitch (suture) and adhesive tape is used to keep the tube in place.
Pleural Chest Tubes • Indications for pleural tube placement: • Hemothorax • Pneumothorax • Pleural effusion • Empyema (drainage of pus) • Postoperative thoracostomy • Allows air to exit the chest and prevents air from entering the chest • Usually inserted at bedside • There are two types of pleural tube connections • Underwater seal drainage • One-way valve
Mediastinal Chest Tubes • Indications for a mediastinal tube include drainage of the mediastinal space after a surgical procedure, cardiac surgery, and creating a pericardial window • No tidaling will be observed with mediastinal tubes due to their location in the mediastinal space as opposed to the pleural space • RN must ensure patency and unobstructed drainage • Inserted in the operating room during surgery
Pre-Insertion Care • Gather the necessary equipment • Instruct client on procedure and expected outcomes • Check for allergies • Administer analgesia and sedation per order • Position client for insertion (semi-Fowlers to high Fowlers depending on reason for insertion) • Assist physician with sterile field & apply mask to self • Assist physician with insertion of chest tube • Place Vaseline gauze dressing around tube at insertion site to prevent air from escaping • Finish with occlusive 4x4 gauze dressing
INSERTION http://www.youtube.com/watch?v=YavZsjsCgVA&feature=related ALL ABOUT http://www.youtube.com/watch?v=y1gaC3yfhvw
Chest Tube Drainage • Chest tube drainage systems act as a one-way valve • Removes pleural drainage • Increases intrathoracic pressure • Decreases chest wall pressure • Restores negative pressure in the lungs • Types of chest tube drainage systems: • Water seal • Dry suction • Water seal drainage system -- • Suction is determined by the amount of water in the water seal system and the amount of suction on the wall • Gentle bubbling sound is expected
Chest Tube Drainage (cont’d) • Dry suction drainage system -- • Closed, one-way drainage system • Orange accordion-like object visible when suction applied • Wall suction controls the rate of air flow • Thoracic pressure is determined by the pressure of the wall suction and the level of the water in the drainage system
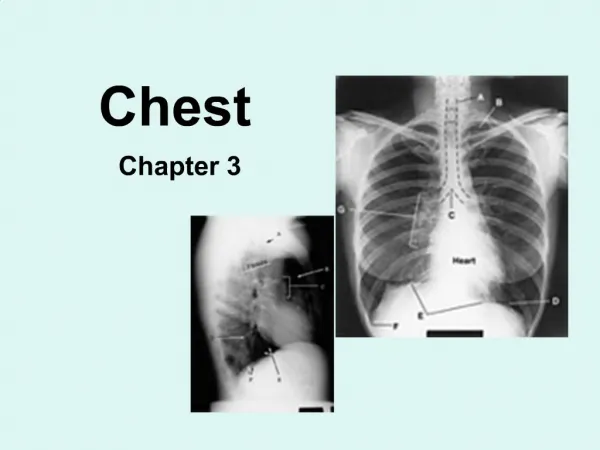
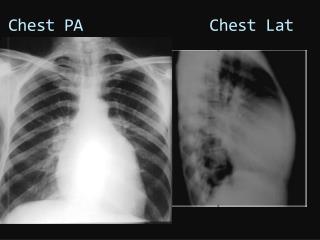
The chest tube usually remains in place until the X-rays show that all the blood, fluid, or air has drained from the chest and the lung has fully re-expanded. • Chest X-Ray Showing a Tension Pneumothorax • See the shifted mediastinum? – the trachea’s shoved over to the right.
Chest Tube Suction • Chest tubes are often connected to suction • Increases drainage • Assists lungs in achieving re-expansion • Chest tube suction is typically set at 20cm (water pressure) • Disconnecting the chest tube from suction does not allow air to enter the chest, but does stop the suction • Indications for removal of chest tube include: • Diminished chest drainage • Frequent re-expansion of the lung • Suction is usually discontinued for a few hours prior to chest tube removal
When the chest tube is no longer needed, it can be easily removed, usually without the need for medications to sedate or numb the patient. Medications may be used to prevent or treat infection (antibiotics).
Post-Insertion Care • Assess the client immediately after insertion and every 4 hours thereafter • Assess vital signs • Check drainage appearance and amount • Should be no greater than 100 mL/h • Record at least every 8 hours • Check chest wall at insertion site for subcutaneous emphysema • Observe for tidaling • Check for kinks in the tubing if none noted • If air bubbles in the air leak indicator are observed, check entire tubing for air leaks
Post-Insertion Care (cont’d) • Ensure suction is set at the ordered level • Make sure drainage system is positioned correctly • Upright and secured • Below the level of the client’s heart • Ensure Vaseline gauze is available at bedside • Make sure client has had a post-insertion x-ray • Change the drainage system receptacle as indicated • Only when chambers are full • Use sterile technique
Tidaling: the middle water seal chamber is observed for expected rise in fluid level with expiration. • Air leak:noted when continuous bubbling is observed in the main water seal chamber • Suction may be wet or dry • A gentle bubbling sound is normal to hear with a wet system • Dry systems have a orange accordion looking object visible when suction is applied • Change the recepticle only when chambers are full using sterile technique • Heimlich Flutter Valve: air and fluid are expelled and not rebreathed in
What is Empyema? • This is a collection of pus in the pleural space, or in a big abscess space in the lung tissue itself. • Pus can collect in large enough quantities to compress the lung, and certainly will act as a septic “focus” until it’s drained. Empyema can result from chest trauma - say, a gunshot or knife wound - or necrotizing pneumonia, or any other process that puts bacteria into the chest.
Chest Tube Complications • Chest tube dislodgement -- • At the chest: • Quickly apply Vaseline gauze (depending on type) to the chest insertion site • Assess for respiratory distress • At the drainage system unit: • Clamp the chest tube while another nurse obtains a new drainage unit • Set up new drainage unit and connect to chest tube • Attempt to complete this entire procedure in less than 1 minute to prevent complications • Clamping a chest tube can result in high risk for developing tension pneumothorax • Risk is increased with positive pressure ventilation
Chest Tube Complications (cont’d) • Assess for chest tube dislodgement at the chest via placing stethoscope over dressing at insertion site and auscultating for whistling sound • Occurs when the chest tube port has dislodged from the chest and is continuously sucking in air from the surrounding atmosphere • Stat x-ray indicated as air may be dangerously re-accumulating in the chest
What if it tips over? • You place the container back in the upright position. Mark the chambers where the blood is or replace chamber if needed. • Check the pt