Download

1 / 15
150 likes | 235 Views
Incentives: Pros and Gone’s The Dryden Experience. DRHC Return of Service Program 1999 crisis hits the community Decisions and factors from the 90’s catch up with a “bulletproof” community History of the Physician Shortage Dryden’s response Success (relative), what’d we learn?

E N D
Incentives: Pros and Gone’sThe Dryden Experience • DRHC Return of Service Program • 1999 crisis hits the community • Decisions and factors from the 90’s catch up with a “bulletproof” community • History of the Physician Shortage • Dryden’s response • Success (relative), what’d we learn? • Hope for the future
Quick History • 90’s mild recession • Provinces slashed health care budgets • “Too many doctors” / Doczone • Restrictive policy deters IMG’s (still? MB/NFLD are progressive) • Outmigration of docs to the US • More female med students (=families 61% NOSM applicants this year) • Burn out ensued, caught us in 2000
Dryden Community Response • Hospital/community/public rallied • Fundraising campaign, raised millions • Bursaries/Return of Service agreements • Bidding war for services ensues • FT recruiter very successful (6 hires) • Staffing levels increase = everyone happy • Storm was coming
Financials • GP – 100,000 for 2 years • GP/ER – 50,000 for 1 year, 80,000 2 year • Spousal assistance • Moving help • 2 years subsidized overhead in the clinic at 20,000/year • All requisite social, housing, recreational and academic supports for family/children
Mass Exodus • 2 FT ER docs, 4 GP’s • All contracts expired b/w July/07-Feb/08 • Chuck hired July 2007 • 6 doctors gone by February/08 • Nice work! • What happened?
Post Mortem • Exit interviews • Profile of the signees • IMG’s working/living in a homogenous community not very diverse (but friendly!) • Spouses dissatisfaction with employment prospects/kids loved the community/ • Distance from family • $$$ elsewhere/Education opportunities offered in larger centre
Public Reaction • Four key considerations • Practice/Life balance • Spousal needs (50%+) • CME/Overhead/Facilities • Community diversity (faith/food/friends/language/culture) • Can’t sell what we don’t have, therefore work on better matches
Renewed Focus • Diligence, match with the community • Shop relatively closer to home • Market in appropriate settings (NOSM/TBay/Sudbury/online/students and resident follow up) • Panel interview process • Don’t be afraid to say no
Revised Results • Hires from regional medical students • Raise profile of bursary program in the region/at nearby med schools • One hire into year 2, has incorporated • One hire starts in August • Local Med Student on bursary (4th year) • Profile amongst students higher • One ER doc from Winnipeg (GP-split practice)
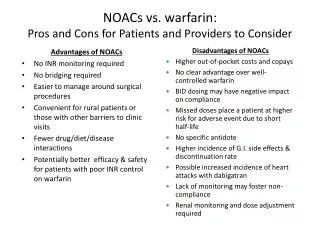
The Problem with Incentives • Expensive! Difficult environment to raise $ • No guarantees – bidding wars • You will attract some people that want to pay bills and leave • Potentially damage support for other hospital initiatives/PR trouble • Reliance on Full Time ER docs in small community shrinks locum pool/local GP support in ER, if they leave…trouble (we nearly closed)
HOPE!!! • Governments moving in right direction to repatriate ex-docs in the U.S. (Canada looks pretty good) • Easy to sell to U.S. Docs, very little billing difficulties with one primary provider to deal with – consider them. • Med students awaiting their J-1 visa applications/citizenship/green card may find Canada an attractive place to practice • Ease restrictions on IMG’s on the horizon • Med School numbers increasing • Communities becoming increasingly creative with local government and private enterprise partnerships
Other Considerations • Community health tax levy to sustain programs for bursaries • Share costs/partner with communities falling in the catchment area of your hospital in rural settings.
Questions? • www.docjobs.ca • schmitt@shaw.ca • I’d be happy to answer any questions, tell you what I know