Download
1 / 41
410 likes | 555 Views
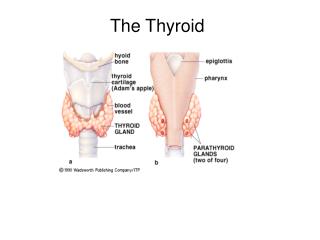
Update on the Thyroid. Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures. Cases . 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4

E N D
Update on the Thyroid Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures
Cases • 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 • 79 yr old man with 1 yr of fatigue and lassitude and no findings except TSH=9.0, anti-TPO positive • 45 yr old women, enlarged thyroid with dominant nodule since 1999, FNA benign. On T4 suppession ever since, TSH=0.1
Thyroid Tests: sTSH • Very sensitive to circulating thyroid hormone levels • Excellent correlation with TRH stimulation (sTSH < 0.1) • Requires intact pituitary-hypothalamic axis;4-6 weeks to equilibrate • Falsely low: severe illness, corticosteriods, dopamine • Normal range 0.5-4.8 mU/L; $58
Thyroid Tests: Free Thyroxine • Measures unbound hormone • Replacing “index” assays • Gold standard: Equilibrium dialysis • Other immunoassays: Improving • Normal range, 9-24 pmol/L; $64
Are Both sTSH and Free T4 Necessary? • American Thyroid Association: Yes • Others recommend sTSH first • UCSF outpatient data • Results when both tests ordered on the same specimen (N=3143) • Each test classified as low, normal or high
Diagnostic Redundancy of sTSH and Free T4 sTSH (mU/L)< 0.5 0.5 - 5.5 > 5.5 < 9 4 16 49 9 - 24 536 2024 309 > 24 174 30 1 Free T4 (pmol/L)
Subclinical Thyroid Disease • Subclinical hypothyroidism“Abnormally high sensitive TSH and normal thyroid hormone levels” • Subclinical hyperthyroidism“Abnormally low sensitive TSH and normal thyroid hormone levels”
Suggested Testing Strategy • If sTSH is normal, STOP • If sTSH is low, measure T4, consider T3 • If sTSH is high, measure T4, consider TPO antibodies
Thyroid Antibodies • Anti-thyroperoxidase, TPO (titer<100, $78) • Similar to “anti-microsomal” • Most sensitive thyroid autoantibody • Specificity a problem • TSH receptor antibody (absent, $112) • Causes Grave’s disease • Rarely found in normal individuals
Thyroid Scans • Technetium 99 ($450) • Low radiation, quick • Useful for nodules in some circumstances • Useful to determine cause of hyperthyroidism • A. High uptake: Grave’s, toxic nodule • B. Low uptake: thyroiditis, thyroxine use
Hyperthyroidism: Epidemiology • Etiology: • Iatrogenic • A. Over replacement (30-50% given rx) • B. Suppression of CA, goiters, and nodules • Autoimmune (Grave’s disease): thyroid stimulating autoantibodies • Autonomous nodule(s). Occasionally T3 • TSH secreting tumors
Hyperthyroidism: Prevalence • Population based prevalence of suppressed TSH:AuthoragemenwomenBagchi (1990) >55 1.8% 2.7%Falkenberg (1991) >60 1.9%Parle (1991) >60 5.5 6.3%Bauer (1993) >55 5.8%
Hyperthyroidism in the Elderly • Weight loss, palpitations, and nervousness less common • Tachycardia, exophthalmos, tremor less common • Atrial fibrillation more common • 8-10% are completely asymptomatic
Subclinical Hyperthyroidism: Cardiac Effects • Systolic time intervals shortened • Clinical significance uncertain • Reduced exercise tolerance • Increased incidence of atrial fibrillation Swain, 1994 Prospective cohort, N = 2000 RR = 3.1 (1.7, 5.5) if sTSH < 0.1
Subclinical Hyperthyroidism: Skeletal Effects • Florid hyperthyroidism causes fractures • Effect on BMD, bone loss controversial • Increased fracture risk (Bauer, 2001)- Prospective study, 9407 older women- TSH < 0.1 vs. normal- Hip fracture: RR = 3.6 (1.0, 12. 9)- Vertebral fracture: RR = 4.5 (1.3, 15.6) • Effect of accelerated bone turnover?
Subclinical Hyperthyroidism: Natural History • Exogenous: Well established • Endogenous: Little longitudinal data Parle, 1991 50 untreated individuals >60 1 developed overt hyperthyroidism After 1 year, sTSH normal in half!
Who Should Be Treated? • Exogenous (iatrogenic) • Dose reduction unless contraindicated • Endogenous (subclinical) • Follow if uncomplicated • Consider treatment if atrial fibrillation or osteoporosis present • Endogenous (overt) • Rule out thyroiditis • Tx everyone else with beta blocker and...
Hyperthyroidism: Treatment • Anti-thyroid drugs (PTU and methimazole) • Remission: 30-50% after 12-18 mo • Side effects: rash, fever, arthritis, agranulocytosis (all rare) • Radioiodine • Best treatment for hot nodules • Remission: everyone • Side effects: transient thyroiditis (rare), hypothyroid (50%), worsening exophthalmous
Radioiodine and Mortality • Franklyn, 1998- 7209 hyperthyroid pts, 15 yr follow-up- All cause mortality: 13% higher than age and sex matched populations- CV deaths increased, but not cancer • Mechanism unknown, clear dose-response • Unable to adjust for other potential confounders
Hypothyroidism: Epidemiology • Etiology • Autoimmune (Hashimoto’s) • Iodine deficiency • Iatrogenic A. Radioiodine/ surgery B. Drugs (lithium, amiodarone) • Pituitary/ hypothalamic disease
Hypothyroidism: Prevalence • Population based prevalence of elevated TSH: Author age men women Tunbridge(1977) >65 6.0% 10.9% Bagchi(1990) >55 1.8% 2.7% Parle(1991) >60 2.9% 11.6%Bauer(1993) >55 5.4%
Overt Hypothyroidism in the Elderly • “Classic” features often missing • Neuropsychiatric complaints common: depression, weakness, memory loss • Other clues: hypercholesterolemia, elevated CK, pleural effusion
Subclinical Hypothyroidism: CV Outcomes • Observational studies • Total cholesterol unchanged, but higher LDL and lower HDL? • What about atherosclerosis? • Rotterdam population-based study (Hak, 2000) • 1149 women, mean age 70 • Subclinical hypo (TSH > 4, nl T4) in 10.8% • Aortic atherosclerosis RR = 1.7 (1.1, 2.6) • History of MI RR = 2.3 (1.3, 4.0)
Meta Analysis of Subclinical Hypothyroidism and CHD Summary OR 1.65 (1.28-2.12) P for heterogeneity: 0.12
Subclinical Hypothyroidism: Other Outcomes • Observational studies of neuropsychiatric symptoms • Conflicting evidence • Four small double blinded trials, sTSH > 5-7 • Randomized to thyroxine or placebo • No significant change in weight, lipids, other laboratory values • Psychometric testing: Treated felt better and had better memory scores
Subclinical Hypothyroidism: Natural History • Many good studies • Spontaneous resolution infrequent • Antibodies strongly influence outcome • If TPO positive, overt hypothyroidism 5%/yr
Hypothyroidism: Treatment • Replace with thyroxine (T4) • T3 + T4 benefit unproven • Typical replacement dose 1.6 mcg/kg • Elderly or CAD: start low (0.025-0.05 mg/d), gradually increase dose • Maintain TSH within the normal range • Wait 6 weeks after dose change • Monitor yearly (noncompliance, reduced T4 clearance)
What About Treatment of Symptomatic but Euthyroid Patients? Forget It. • Symptoms of hypothyroidism common • Real but not detected by usual tests? • Double blind RCT (Pollock, 2001) • 25 “symptomatic”, 18 “controls” • All euthyroid • 3 mo of T4 (0.1/d) or placebo, cross-over • TSH fell with T4 tx but no difference in cognitive or psychological function
Thyroid Nodules: Epidemiology and Evaluation • Nodules are common (and cancer is rare) • 90% women over age 60 have one or more thyroid nodules at autopsy • Risk factors for cancer: neck irritation, FH • Evaluation: FNA first • 75% benign, 20% suspicious, 5% malignant • Best centers: false negative 2% false positive 1%
Thyroid Nodules: Treatment • Cancer- Histology is important (papillary best)- Surgery and 131I ablation - Suppression with T4? TSH = 0.1-0.4 • Benign nodules- Many shrink spontaneously- Meta analysis of T4 suppression Smaller: 26% vs. 12% (NNT=7) Larger: 8% vs. 17% (NNT=11)- T4 doesn’t prevent new nodules
Screening Cost-effectiveness • Danese and Sawin, 1995 • Cost-utility analysis, sTSH-based screening • Modeled progression, symptoms and CAD • Screening every 5 year from 35-65: $9,223 per QALY in women $22,595 per QALY in men • Sensitivity analysis: cost of TSH key ($25)
Screening for Subclinical Thyroid Disease • US Preventive Task Force, 1996“Routine screening is not recommended. Insufficient evidence for high risk patients, including elderly.” • ACP, 1998“It is reasonable to screen women older than 50 years of age for unsuspected but symptomatic thyroid disease.”
Screening Cost-effectiveness • Effects on HDL, fractures not included. Cost of testing overestimated ($3/TSH) • Published analyses underestimatecost-effectiveness • Other unresolved issues: • Age to start screening? • Optimal frequency?
Summary Take Home Points • sTSH is best test • Subclinical thyroid disease is common, associated with morbidity, and treatable • Low threshold to treat subclinical hypo • Treatment threshold for subclinical hyper less certain • Screening with sTSH is cost-effective
Cases • 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 • 79 yr old man with 1 yr of fatigue and lassitude and no findings except TSH=9.0, anti-TPO positive • 45 yr old women, enlarged thyroid with dominant nodule since 1999, FNA benign. On T4 suppession ever since, TSH=0.1