Download
1 / 34
360 likes | 826 Views
THE THYROID GLAND. HYPOTHYROIDISM. DIRECT METHODS Circulating levels of total hormones total thyroxine (TT 4 ) total triiodothyronine (TT 3 ) protein bound iodine (PBI) Circulating levels of free hormones free thyroxine (fT 4 ) free triiodothyronine (fT 3 )

E N D
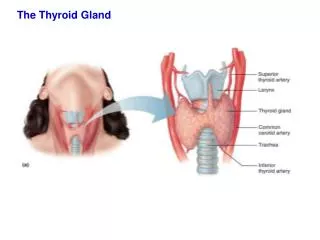
THE THYROID GLAND HYPOTHYROIDISM
DIRECT METHODS Circulating levels of total hormones total thyroxine (TT4) total triiodothyronine (TT3) protein bound iodine (PBI) Circulating levels of free hormones free thyroxine (fT4) free triiodothyronine (fT3) Thyroid hormone binding proteins Thyroxine binding globulin (TBG) INDIRECT METHODS Thyroid hormone binding tests resin uptake of 125I-T3 Free thyroxine index (FTI) FTI= MEASUREMENT OF THYROID HORMONES T4 x patient 125I-T3 resin uptake Control 125I-T3 resin uptake
Dynamic tests of thyroid activity Thyroid uptake of 123I or 131I (and scan) Thyroid uptake of 99mTc T3 suppression test TSH stmulation test Tests of the thyroid-pituitary axis Basal serum TSH Serum TSH response to exogenous TRH OTHER TESTS OF THYROID FUNCTION exaggerated response - hypothyroid normal response - euthyroid impaired response - hyperthyroid
HYPOTHYROIDISM Hypothyroidism is a disease caused by a level of thyroid hormone insufficient for normal body function. It affects every cell of human body. An enlarged thyroid gland is the abnormality present in most cases.
HYPOTHYROIDISM PRIMARY /thyroid gland/ Causes of hypothyroidism SECONDARY /pituitary/ TERTIARY /hypothalamus/
CONGENITAL Athyreosis Ectopic thyroid Dyshormonogenesis Iodide deficiency Antithyroid immunity (transient due to illness) ACQUIRED Iodine deficiency Autoimmunity Post-radioactive iodine therapy Post-thyroidectomy Antithyroid drugs (e.g. Carbimazole) Iodine excess Subacute thyroiditis Thyroid irradiation Primary hypothyroidism
Secondary hypothyroidism pituitary tumours pituitary granulomas (e.g. sarcoid) or injury „empty sella” syndrome Tertiary hypothyroidism • hypothalamic disorders (e.g. craniopharyngioma) • Isolated TRH deficiency
CAUSES OF HYPOTHYROIDISM • Iodine deficiency is the most common cause of goitre and bordeline hypothyroidism worldwide. • In noniodine-deficient areas autoimmunity is the common cause of hypothyroidism
EFFECTS OF IODINE DEFICIENCY Goitre, rarely hypothyroidism EXCESS, ACUTE Temporary inhibition of thyroid hormone synthesis (Wolff-Chaikoff effect) Induction of thyrotoxicosis (Jod-Basedow phenomenon) EXCESS, CHRONIC Goitre, hypothyroidism
REDUCTION OF DIETARY IODINE INTAKE thyroid hormone production (preferential secretion of T3 rather than T4) compensatory TSH secretion IODINE DEFICIENCY
MODERATE Urinary iodide excretion: 25 -50μ/g creatinine Prevalence of goitre: 20 -50% Hypothyroidism: rarely SEVERE Urinary iodide excretion: <25μ/g creatinine Prevalence of goitre: >50% Hypothyroidism: frequently IODINE DEFICIENCY
EXCESS OF IODINE Acute increase in intracellular iodine concentrations Temporal inhibition of thyroid hormone synthesis and release (Wolff-Chaikoff effect) Decrease in intracellular iodine concentration (escape from Wolff-Chaikoff effect)
EXCESS OF IODINE Introduction of iodine therapy in areas of iodine deficiency Increase in the frequency of thyrotoxicosis (Jod-Basedow phenomenon) unmasking thyroid autonomy (previously protected by iodine deficiency)
EXCESS OF IODINE Prolonged iodine ingestion in patients with autoimmune thyroiditis (Hashimoto’s disease) and in fetal and neonatal period (maternal ingestion of excess iodine) Permanent hypothyroidism and goitre formation No excape from Wolff-Chaikoff effect
CLINICAL PICTURE OF HYPOTHYROIDISM DEPENDS ON TIME OF THE ONSET OF DISEASE
CONGENITAL HYPOTHYROIDISM • The prevalence: 1 : ~4,000 live births • Usually no signs at birth • Untreated congenital hypothyroidism Non-reversible retardation of physical and mental development
Typical face Macroglossia Enlarged posterior fontanelle (>0.5 cm) N Hypotonia Hypoactivity Mottled skin Cold extremities Dry skin Umbilical hernia (>0.5cm) N Delayed passage of meconium N Constipation Feeding problems Prolonged icterus N Hoarse, grunting cry Goiter Placidity, lethargy Growth retardation and immature body proportions Mental retardation Clinical features of congenital hypothyroidism N – symptoms only observed in the neonatal period All signs are facultative and frequently are not seen in the neonatal phase.
CONGENITAL HYPOTHYROIDISM • May be detected biochemically by screening all neonates 3 – 5 days after birth. T4 screening TSH screening Prematurity Low TBG Laboratory error False positive Laboratory error Hypopituitarism Laboratory error Ectopic thyroid Laboratory error False negative
ACQUIRED HYPOTHYROIDISM • In noniodine-deficient areas primary hypothyroidism women : men = 10 : 1 • The prevalence in women of all ages: 2 - 4% (one-third of this cases iatrogenic hypothyroidism)
ACQUIRED HYPOTHYROIDISM CLINICAL FEATURES IN HYPOTHYROIDISM The symptoms of hypothyroidism are nonspecific and may be attributed by both patient and doctor to ageing, the onset usually being insidious.
USUAL Lethargy Increased sleep Constipation Mild weight gain Cold intolerance Facial puffiness Dry skin Hair loss Hoarsensess Abnormal menses Acroparaesthesiae Snoring RARE Deafness Psychosis Cerebellar disturbance Myotonia Symptoms of hypothyroidism
Change in appearance (e.g. face puffy and pale) Periorbital oedema Dry, flaking, cool, pasty skin Diffuse hair loss Bradycardia Signs of median nerve compression (carpal tunnel syndrome) Effusions in body cavities (e.g. ascites, pericardial effusion) Delayed relaxation of reflexes Croaky voice Goitre Rarely stupor or coma SIGNS OF HYPOTHYROIDISM
MYXOEDEMA Myxoedema is a severe form of hypothyroidism causing complete exhaustion of all bodily functions. All the organs are infiltrated with mucopolysaccharides that interfere with proper cell metabolism. Myxoedema patients have all the symptoms and signs described for hypothyroidism, as well as low brain center reserve, low cardiac reserve, low respiratory reserve, low adrenal reserve, and low thermoregulatory reserve. In addition, they may show hyponatremia, hypercapnia, hypoxia, and anemia.
HYPOTHYROIDISM- DIAGNOSTIC PROCEDURES • TSH level (second or third generation assays = the lower detection limit: 0.05-0.005 -0.002 mU/l) • FT4 level (the measurement of T3 is not a good diagnostic test for hypothyroidism) • TSH response to exogenous TRH (secondary and tertiary hypothyroidism; subclinical hypothyroidism)
Primary Hypothyroidism Secondary Hypothyroidism Tertiary Hypothyroidism Non-thyroid illness Basal TSH raised low or normal low, normal or elevated normal or low Hypothyroidism- summary of diagnostic tests T4 low low low low TRH response exaggerated reduced or absent sluggish or delayed normal or low
Subclinical hypothyroidism(diminished thyroid reserve) Serum T4 : normal (lower half of the normal range) Serum T3: normal or sometimes even slightly elevated Basal TSH: slightly raised TSH/TRH: exaggerated Definition: „subclinical” no symptoms and signs (?) Patients with subclinical hypothyroidism are at increased risk for coronary heart disease HOWEVER
IMAGING STUDIES • Rapidly growing large goiter; • Goiter with a dominant nodule; • Hashimoto’s disease ultrasonography examination and fine needle aspiration biopsy
IMAGING STUDIES • Cardiac function shoud be assessed before treatment is started. • The presence of other associated autoimmune endocrinopathies must be ascertained.
HYPOTHYROIDISM –TREATMENT • Hypothyroidismis treated with replacement T4 therapy (sodium L-thyroxine) • Replacement doses usually start at 50 μg/d being increased in a stepwise fashion at monthly intervals to 100 - 150 μg/d as the response is assessed clinically and biochemically.
HYPOTHYROIDISM –TREATMENT • There is considerable variation in patient response to T4 because of differential thyroid hormone receptor isoform tissue concentration.
HYPOTHYROIDISM –TREATMENT During T4 therapy: • Serum T3 concentration must be in the normal range, as should that of TSH • Serum T4 may exceed the upper limit of normal.
HYPOTHYROIDISM –TREATMENT During T4 therapy: • Clinically satisfactory response: • normal pulse rate • and complete resolution of presenting symptoms and signs. • Occasionally cardiac symptoms such as palpitations may occur; in this case a β-adrenergic blocker drug is indicated.
HYPOTHYROIDISM –TREATMENT In patients with ischemic heart disease: • Replacement therapy should be introduced cautiously, with started doses of 25μg/d; increments should also be small.
Take blood for diagnostic tests: T4, TSH and plasma cortisol Give 300 μg T4 i.v. and repeat approximately 100 μg q.d; give via nasogastric tube if i.v. preparation is unaviable Treat hypothermia with gradual rewarming using blankets Give i.m. hydrocortisone 75 mg immediately and repeat 25-50 mg 8-hourly Give T3 20 μg i.v., i.m. or by nasogastric tube 12-hourly, if possible Treat any heart failure with diuretics Correct any electrolyte disturbances Carefully exclude or treat infection Use sedative drugs and fluids sparingly Measure serum T4, T3 and TSH frequently Protocol for the management of myxoedema coma