Download
1 / 48
500 likes | 763 Views
CT Perfusion in acute ischemic stroke and the PLEASE No CTP trial. Ameer E. Hassan DO, Clinical Director of Endovascular Surgical Neuroradiology, Neurocritical care and Clinical Neuroscience Research, Valley Baptist Medical Center Assistant professor, Neurology and Radiology

E N D
CT Perfusion in acute ischemic stroke and the PLEASE No CTP trial Ameer E. Hassan DO, Clinical Director of Endovascular Surgical Neuroradiology, Neurocritical care and Clinical Neuroscience Research, Valley Baptist Medical Center Assistant professor, Neurology and Radiology University of Texas Health Science Center – San Antonio
Financial: • Consultant for GE Healthcare, Microvention and Covidien. • Conflicts of interest: none Disclosures
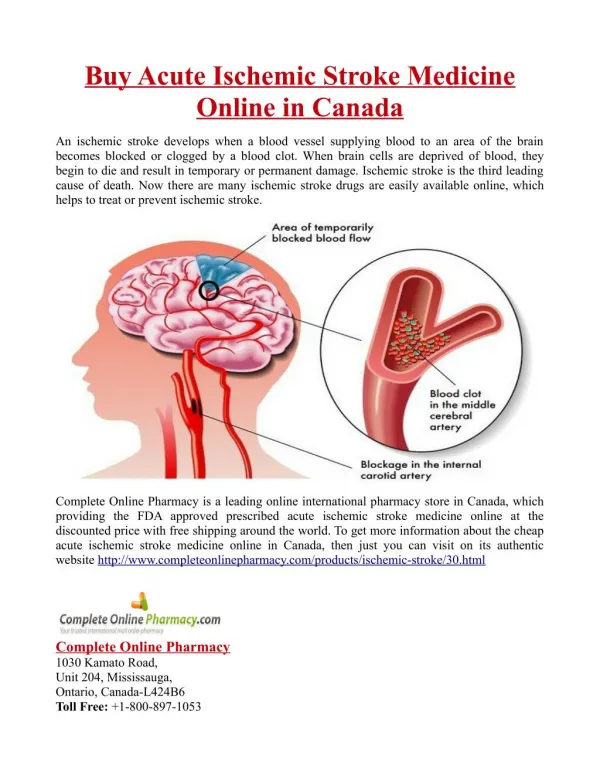
Non-contrast cranial computed tomographic (CT) scan findings in acute ischemic stroke patients have been classically used to select patients for intravenous and endovascular thrombolysis therapy in the: • European Cooperative Acute Stroke (ECASS) I1,II2 and III3, • Interventional Management of Stroke (IMS) I4,II5 and III6, • Prolyse in Acute Cerebral Thromboembolism (PROACT) II7, • Mechanical Embolus Removal in CerebralIschemia (MERCI)8 trials. Background
Studies have found that dynamic CT-P images were more accurate than non-enhanced cranial CT in the detection of ischemic stroke in patients presenting with symptoms less than 12 hours in duration. • Anotherstudyfoundthat CT perfusion (CT-P) imaging was more sensitive [100%] and specific [92%] than non contrast CT [93% sensitive and 67% specific] for the detection of large ischemic infarcts (affecting greater than one third of the affected lobe). • Subsequently, new emphasis has been placed on using CT-P imaging to select patients with acute ischemic stroke who can benefit from an expanded time window with intravenous or endovascular treatment. Background
??? Expanding the time window after 4.5 hours
Arrival 15 minutes 25 minutes 45 minutes 60 minutes & within 4.5 hours of onset Not defined Endovascular time window What can we offer our patients? Expanding the time window after 4.5 hours
Trend of thrombolytic use in the United States Hassan AE, Chaudhry SA, Grigoryan M, Tekle WG, Qureshi AI. Stroke. 2012 Nov;43(11):3012-7.
Based on analysis of the Nationwide Inpatient Sample database from 2005 to 2008: • intra-arterial thrombolysis has steadily increased by 17%, 22%, 25% and 35% respectively. • However the proportion of patients who are disabled or dead has not changed over the years. • Patients discharged to a nursing facility are still around 49% and approximately 14% of patients die in the hospital. Trend of thrombolytic use in the United States (Hassan et al. Stroke 2012)
While endovascular treatment has reduced the rate of death and disability compared with no treatment • The relatively high rate and expense associated with such treatment mandates a more effective strategy for patient selection. Endovascular Thrombolysis
In order to increase the rates of good outcomes, new emphasis has been placed on using advanced neuroimaging to select patients with acute ischemic stroke who can benefit from endovascular treatment. • The potential of CTP is based on high prevalence of use among patients with acute stroke to confirm the diagnosis of ischemia without delaying treatment. Endovascular Thrombolysis
The presence of ischemic penumbra on CT-P can be identified based on: • increased mean transit time (MTT), • decreased cerebral blood flow (rCBF), and • normal or increased cerebral blood volume (rCBV)11 • All potentially used to select acute ischemic stroke patients for intravenous12 or endovascular treatment. CTP Selection of Penumbra
increased mean transit time (MTT), decreased cerebral blood flow (rCBF), and normal or increased cerebral blood volume (rCBV)
There are limitations to acquisition and interpretation of CT-P imaging. • Multi-slice CT scanners provide 2 to 4 cm of coverage per acquisition which do not always allow the evaluation of the exact perfusion deficit volumes if they exceed the volume studied.12 • The variation in reconstruction of CT-P images and qualitative interpretation of salvageable tissue may lead to selection of a relatively heterogeneous population, leading to the inclusion of patients with limited salvageable tissue which may obscure the benefit of endovascular treatment. • False negatives and un-interpretable imaging can be obtained when using CT-P imaging largely due to a patient’s low cardiac output, inappropriate slow rate of bolus administration, contrast extravasation in the subcutaneous tissue, patient movement, and operator inexperience.11 Limitations of CTP
Endovascular treatment patient selection: • ≤ 4.5 hours • NIHSS of ≥10 • 4.5-6 hours • NIHSS of ≥10 • NIHSS <9 with mismatch on perfusion • 6-24 hours • NIHSS of ≥10 • Anterior circulation • if large perfusion mismatch is present • All basilar artery occlusions within the first 24 hours Current Endovascular Protocol
Protocol for acute ischemic stroke treatmentTime dependent loss of benefit Value of Additional imaging salvage-able brain 0-3 hrs Ischemic stroke 3-6 hrs >6 hrs
Time dependent value of additional imaging-Identify presence of salvageable tissue.(Hassan AE. Stroke. 2010 Aug;41(8):1673-8) rCBF-rCBV mismatch on CTP Salvageable tissue Time
Time dependent value of additional imaging-Identify presence of salvageable tissue.(Hassan AE. Stroke. 2010 Aug;41(8):1673-8) Diffusion-perfusion mismatch on MRI OR rCBV-rCBF mismatch on CTP Salvageable tissue rCBV + rCBF↓ Time
CTP Guided and Time Guided Endovascular Treatments (Re: Hassan AE. Stroke. 2010 Aug;41(8):1673-8) CTP guided endovascular treatment did not increase the rate of short-term favorable outcomes among acute ischemic stroke patients
So if CTP should select patients for endovascular treatment more appropriately, what happened? Limitations of CTP
Kappa values for the treatment decisions based on CT images was 0.43 (range 0.14-0.8) (moderate agreement), and for the decisions based on CTP images was 0.29 (range 0.07-0.67) (fair agreement) among the five subjects. • There was substantial variability within the group and between images interpretation. • Observed agreement on decision to treat with endovascular therapy was found to be 75% with CT images and 59% with CT-P images (with no adjustment for chance). Kappa values for intra-rater agreement were -0.14 (ranged -0.27-0.27) (poor agreement). • In conclusion, there is considerable lack of agreement, even among stroke specialists, in selecting acute ischemic stroke patients for endovascular treatment based on CT-P changes. This mandates a careful evaluation of CT-P for patient selection before widespread adoption. Agreement and variability in the interpretation of presenting CT and CT-Perfusion Imaging changes in Ischemic Stroke Patients qualifying for endovascular therapy.(Hassan et al. NeurocritCare. 2012 Feb;16(1):88-94.)
CT-P example of a Right MCA stroke with the majority of reviewers deciding to treat with endovascular therapy Agreement and variability in the interpretation of presenting CT and CT-Perfusion Imaging changes in Ischemic Stroke Patients qualifying for endovascular therapy.(Hassan et al. Neurocrit Care. 2012 Feb;16(1):88-94.)
CT-P and CT scan example of a Left MCA stroke with the majority of reviewers deciding NOT to treat endovascularly. Agreement and variability in the interpretation of presenting CT and CT-Perfusion Imaging changes in Ischemic Stroke Patients qualifying for endovascular therapy.(Hassan et al. Neurocrit Care. 2012 Feb;16(1):88-94.)
A randomized multicenter trial (22 stroke centers) with a total of 118 patients from 2004 to 2011. • Embolectomy was not superior to standard care in patients with either a favorable penumbral pattern (mean score, 3.9 vs. 3.4; P=0.23) or a nonpenumbral pattern (mean score, 4.0 vs. 4.4; P=0.32). • In the primary analysis of scores on the 90-day modified Rankin scale, there was no interaction between the pretreatment imaging pattern and treatment assignment (P=0.14). A trial of imaging selection and endovascular treatment for ischemic stroke. (MR RESCUE Investigators, NEJM, March 2013)
A favorable penumbral pattern on neuroimaging did not identify patients who would differentially benefit from endovascular therapy for acute ischemic stroke, nor was embolectomy shown to be superior to standard care. A trial of imaging selection and endovascular treatment for ischemic stroke. (MR RESCUE Investigators, NEJM, March 2013)
Interventional Management of Stroke III (IMS III) – Broderick JP et al. N Engl J Med. 2013 Mar 7;368(10):893-903. • Phase III, randomized, multi-center, open-label clinical trial • Purpose: To determine whether a combined IV/IA approach to recanalization is superior to standard IV rt-PA alone when initiated within 3 hours of stroke onset. • Primary outcome measure: Favorable outcome in terms of functional independence as measured by a Modified Rankin Scale score of 0-2 at 3 months. IMS III Prematurely terminated because it passed the point of significance even if the trial was completed
RCT of 656 patients with documented large-artery occlusions, NIHSS 8 or higher: • 434 randomized to EST after bridging (low-dose) IV t-PA; • 222 randomized to full dose IV t-PA; • Results: no difference in outcomes between the two groups overall, despite a hint of the appropriate shift in mRS favoring EST: Endovascular Interventions - Interventional Management of Stroke III (IMS III)
Good reperfusion (TICI 2b or 3) was achieved in only 44% of patients with an M1 occlusion, and at a similar or lower rate for other sites of occlusion; • In keeping with previous literature reports, IV TPA does not seem to work well for stroke due to carotid terminus occlusions or tandem extracranial ICA/M1 occlusions. • In IMS3 the rate of good outcome in these patients was 4%. With IV/IA outcomes a bit better (26%) but overall remain poor. At our center, about 20-30% of patients we treat fall into this category. This is not a small minority of patients! Endovascular Interventions - Interventional Management of Stroke III (IMS III)
EST used IA t-PA or any approved thrombectomy device the treating physician chose to use: • IA t-PA only (n=151) • MicroSonic SV system (n=14) • 20% with no lesion to treat • Merci (n=77) { <18% of total EST patients} • Penumbra (n=39) { <10% of total EST patients} • Solitaire (n=4) { <1% of total EST patients} Endovascular Interventions - Interventional Management of Stroke III (IMS III)
Learning points (ISC 2013, Honolulu HI ): • Largest signals in favor of EST are: Terminal ICA occlusions, severe deficits (NIHSS>20) and early time to treatment. • Reperfusion is a good thing, but it is TIME dependent, for every 30 minute delay in reperfusion there is a 10% lower chance of a good outcome • MERCI has more associated complications than other EST approaches. • Centers like University of Cincinnati (PI of IMS I, II, & III) still practice the same approach prior to IMS III results. • Majority of EST at large centers includes IV TPA excluded patients (recent major surgery, INR > 1.7, previous intracranial pathology, etc.), posterior circulation occlusions, and OUTSIDE of the time window; AS WELL AS patients with M1 occlusions who are not improving within first 30 minutes of IV TPA. Endovascular Interventions - Interventional Management of Stroke III (IMS III)
Comparing EST to proven MI treatment: • In acute MI, many of the original trials comparing endovascular therapy to IV lytics were negative and even the latest trials comparing endovascular therapy to IV fibrin-specific lytics had a difference of 1% mortality (which required pooled analyses and large sample sizes). • The reality of endovascular acute stroke care (including at top academic centers in the US) during IMS3 was conducted is one of long delays from hospital presentation to groin puncture (mean 81 min from iv t-PA administration to groin puncture and another 42 min from groin to treatment start in IMS3). • Contrast this to the mandatory door to ballon time of 90 minutes in acute coronary syndromes beyond which Medicare does not reimburse acute coronary interventions for MI and you can appreciate where we stand compared to our cardiology colleagues. • In fact whenever a cardiologist asks me why all those trials published in the New England Journal of Medicine were negative my answer is "imagine a percutaneous coronary revascularization trial against IV lytics in which the door-to-balloon time is 3 hours and you will understand why." Endovascular Interventions - Interventional Management of Stroke III (IMS III)
A recent retrospective multicenter analysis (10 stroke centers) with a total of 556 treated with endovascular thrombolysis showed that multimodal imaging was associated with delays in treatment without reducing hemorrhage rates or improving clinical outcomes. • 286 (51%) patients had a non-contast CT, 190 (34%) patients had CT-P, and 80 (14%) patients had MRI. Advanced modality imaging evaluation in acute ischemic stroke may lead to delayed endovascular reperfusion therapy without improvement in clinical outcomes. (Sheth et al. JNIS, May 2013)
Non contrast CT had significantly lower median times to groin puncture (61 min, IQR 40-117), compared with CTP (114 min, 81-152) or MRI (124, 87-165). • They concluded that a prospective trial is warranted to support advanced imaging. Advanced modality imaging evaluation in acute ischemic stroke may lead to delayed endovascular reperfusion therapy without improvement in clinical outcomes. (Sheth et al. JNIS, May 2013)
2013 AHA/ASA Guidelines for Early Management of Patients With Acute Ischemic Stroke • CT perfusion and MRI perfusion and diffusion imaging, including measures of infarct core and penumbra, may be considered for the selection of patients for acute reperfusion therapy beyond the time windows for intravenous fibrinolysis. (Class IIb; Level of Evidence B)” Definitions Class IIb:Usefulness/efficacy is less well established by evidence or opinion Evidence B: Greater conflicting evidence from single randomized trial or nonrandomized studies Evidence based guidelines
To demonstrate that non-contrast computed tomography imaging within 8 hours of acute ischemic stroke symptom onset is comparable to computed tomography perfusion imaging. Objective
We will prospectively study all consecutive acute ischemic stroke patients who are treated within 8 hours of symptom onset with an endovascular intervention. In the setting of wake up strokes, time of symptom onset is identified by time last seen normal. Methods
All the patients will undergo, non-contrast computed tomography imaging, computed tomography angiography and computed tomography perfusion imaging. • The endovascular treatment team will be blinded to the results of the computed perfusion imaging. • Every patient will undergo non-contrast computed tomography 24 hours and 48 hours post endovascular intervention as well as after any suspected deterioration in neurologic function. Methods
Additional Data Collected: • age and gender • pre-admission vascular risk factors (hypertension, dyslipidemia, diabetes mellitus, cigarette smoking, atrial fibrillation, congestive heart failure, history of stroke/TIA and coronary artery disease) • race/ethnicity • Pre- and intra- procedural intubation status will be obtained. • Data regarding severity of stroke will be quantified by the admission National Institutes of Health Stroke Scale (NIHSS) score and discharge functional outcome was ascertained using the modified Rankin Scale (mRS) score. Methods
The stroke team will use the ASPECTS method to read the CT scans. • The ASPECTS is determined from two standardized axial CT cuts, one at the level of the thalamus and basal ganglion and one adjacent to the most superior margin of the ganglionic structures, such that they were not seen. • On these two sections, which are, by definition, not continuous, the MCA territory is allotted 10 points. • A single point is subtracted for an area of early ischemic change, such as focal swelling or parenchymal hypoattenuation, for each of the defined regions. • A normal CT scan receives an ASPECTS of 10 points. A score of zero indicated diffuse ischemic involvement throughout the MCA territory. CT Protocol - ASPECTS
New focal neurological signs in the Internal carotid artery, Middle Cerebral Artery, or Anterior Cerebral artery distribution allowing initiation of treatment within 8 hours of the onset of symptoms; • A minimum National Institutes of Health Stroke Scale (NIHSS) score of 8 • Age greater than or equal to 18 years. Inclusion Criteria
NIHSS score greater than 30 • coma • Rapidly improving neurological signs at any point prior to endovascular intervention • Seizures at onset • Clinical presentation suggestive of subarachnoid hemorrhage • Septic embolism • Suspected lacunar stroke • Active or recent hemorrhage within 30 days • Known hemorrhagic diathesis • Baseline international normalized ratio greater than 3 • Receipt of heparin within 48 hours with a partial thromboplastin time greater than two times the lab normal • Platelets less than 30,000 • Sustained severe hypertension • Evidence of intracranial hemorrhage, significant mass effect with midline shift, or an obvious infarction of greater than one third (100mls) of the Middle Cerebral Artery vascular territory on non-contrast head computed tomography scan Exclusion Criteria
24 hour NIHSS score following treatment • 7 day or discharge NIHSS score • Discharge modified Rankin score • In-hospital mortality • Symptomatic intracranial hemorrhage, andasymptomatic intracranial hemorrhage rates. Primary Outcomes
The perfusion scans obtained will be generated using both Gaussian Fit and single value deconvolution methods using Vitrea software (Vital Images), yielding the following perfusion parameters: time to peak, MTT, rCBF, and rCBV. • The CT-P scans will be retrospectively reviewed by a neuro-radiologists and two endovascular interventionalists to determine which patients have a penumbra (preserved rCBV, decreased rCBF and increased MTT) and would have been appropriate for an endovascular intervention. • Inter-observer agreement will be determined. CTP analysis
Based on qualitative analysis of the cerebral blood volume maps, we will define salvageable tissue (penumbra) amenable to endovascular intervention, to be present when the total ischemic territory is at least 20% greater than the infarcted area and the ischemic zone involved the cortex. • In the case of an MCA vascular territory infarction, the patient will be excluded from intervention if the infarct burden is greater than or equal to one third of the vascular territory on qualitative analysis of the CT-P cerebral blood volume (CBV) map. • The CT-P infarct core and ischemic penumbra will be automatically calculated by the software using the appropriate MTT and rCBV thresholds (CT-P penumbra: MTT >145% of the contralateral side values, rCBV > 2 mL/100 g; CT-P infarct: MTT >145% of the contralateral side values, rCBV <2 mL/100 g). CTP analysis
A total of 102 patients have been screened for this trial over a 2 year period at 2 stroke centers. • A total of 55 patients have been enrolled • 47 patients were excluded: • Posterior circulation • No CTP performed • Not consentable or did not want to sign consent • Last seen normal >8 hours • NIHSS<8 Results
Acute ischemic stroke Comprehensive treatment growth Comprehensive Stroke Service
Time is brain, The availability of endovascular interventions should notpreclude the IV TPA in eligible patients • CTP guided endovascular treatment has not been associated with improved outcomes among acute ischemic stroke patients in the current literature (most likely due to delay in treatment). • Prospective studies are required to validate the CTP criteria and protocols currently in use, while using the latest stroke devices (Solitaire, Trevo, and Penumbra) prior to incorporating CTP as a routine patient selection modality for acute ischemic stroke treatments. Conclusion