Download
1 / 53
1.5k likes | 3.25k Views
UPDATE IN ACUTE ISCHEMIC STROKE MANAGEMENT. DLG DISCLOSURES. FINANCIAL DISCLOSURE I have no financial relationships or affiliations to disclose. UNLABELED/UNAPPROVED USES DISCLOSURE

E N D
DLG DISCLOSURES • FINANCIAL DISCLOSURE • I have no financial relationships or affiliations to disclose. • UNLABELED/UNAPPROVED USES DISCLOSURE • I will reference the following off-label or investigational use of drugs or products: intra-arterial t-PA in stroke patients
STROKE IN THE UNITED STATES Affects > 780,000 persons per year Major cause of death (#3) & long-term disability Oklahoma has 6th-highest stroke death rate Estimated U.S. cost for 2008 = $65.5 billion Mostly hospital (esp. LOS) & poststroke costs Appropriate use of IV t-PA s long-term cost DRG 559 for AIS w/ thrombolysis ( hospital reimbursement from $5k to $11.5k)
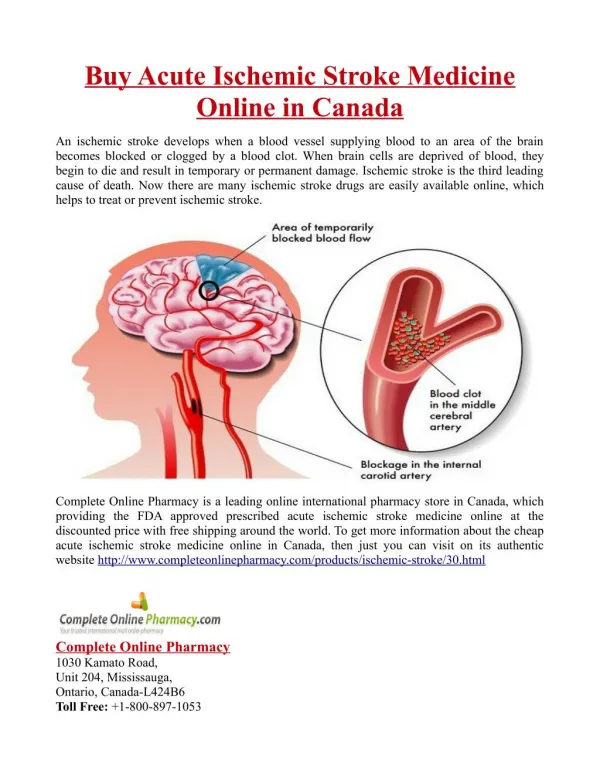
THREE STROKE TYPES Focal Brain Dysfunction Intracerebral Hemorrhage Bleeding into brain Subarachnoid Hemorrhage Bleeding around brain Ischemic Stroke Clot occluding artery 85% 10% 5% Diffuse Brain Dysfunction
INFARCT CLOT ACUTE ISCHEMIC STROKE (AIS) & TIALOW BLOOD FLOW TO FOCAL AREA OF BRAIN • Pathophysiology: • Usually thromboembolism (blood clot forms in vascular system, travels downstream, plugs cerebral artery) • Acute therapy: • Thrombolysis (or thrombectomy) • Do NOT lower BP • Avoid aspiration / IV glucose • 2 prevention: • Antithrombotic therapy • Vascular risk factor therapy • Possible carotid endarterectomy (CEA) or angioplasty (CAS) Ischemic stroke= Infarction with sequelae Transient ischemic attack= No infarction and no sequelae
TRANSIENT ISCHEMIC ATTACK (TIA) AND “ACUTE NEUROVASCULAR SYNDROME” • Transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia, without infarction • Typically < 1 h, but time limit is no longer part of definition • Risk of stroke = 5% w/in 2 d, 10% w/in 3 m • Appropriate antithrombotic therapy based on cause • Urgently evaluate for cause • MRI w/ DWI, intracranial MRA, carotid duplex, echo • Can admit to “observation status” Discover cause, determine therapy, decrease risk!
Penumbra Core Clot in Artery ISCHEMIC STROKE PATHOPHYSIOLOGYThe First Few Hours “TIME IS BRAIN: SAVE THE PENUMBRA” Penumbra is zone of reversible ischemia around core of irreversible infarction—salvageable in first few hours after ischemic stroke onset Penumbra damaged by: • Hypoperfusion • Hyperglycemia • Fever • Seizure
Penumbra Core CEREBRAL BLOOD FLOW (ml/100g/min) Normal function 20 15 Neuronal dysfunction CBF 8-18 PENUMBRA 10 Neuronal death CBF < 8 5 CORE 1 2 3 TIME (hours) ISCHEMIC PENUMBRA: PATHOPHYSIOLOGYOF THERAPEUTIC WINDOW Identification of penumbra through MRI perfusion-diffusion mismatch or perfusion CT may replace time as the major indication for emergency acute ischemic stroke therapies.
ORGANIZED CARE OF STROKE PATIENTS:PERFORMANCE IMPROVEMENT / UTILIZATION REVIEW • Acute stroke team • Stroke multidisciplinary team • Stroke unit • Prewritten stroke orders • Address each aspect of care each day Supportive medical care Treatment of acute stroke Rehabilitation Outpatient planning Keep away future strokes Etiologic evaluation An organized approach enables emergency treatment, a thorough evaluation, and improved patient outcome at decreased cost. Stroke unit care results in decreased rate of aspiration pneumonia, decubiti, stroke progression or recurrence, and death.
Acute (4 hours) Infarction Subacute (4 days) Infarction R L L R Subtle blurring of gray-white junction & sulcal effacement Obvious dark changes & “mass effect” (e.g., ventricle compression) STROKE EMERGENCY BRAIN IMAGING:NONCONTRAST CT SCAN
STROKE EMERGENCY BRAIN IMAGING:NONCONTRAST CT SCAN Intracerebral Hemorrhage Subarachnoid Hemorrhage CT detects 90% of SAHs; if SAH suspected & CT negative, must LP CT detects all ICHs immediately
< 3.0 Hours No upper age limit No limit on stroke size Can give if taking warfarin & INR < 1.7 3.0-4.5 Hours Do NOT give if: Pt > 80 yo NIHSS > 25 DM w/ previous stroke Taking warfarin at all AIS EMERGENCY THERAPY: IV TISSUE PLASMINOGEN ACTIVATOR (T-PA) • Must give < 4.5 h—earlier you give it, better the outcome • Stroke onset = last time known to be normal • Do NOT give if glucose < 50 • Do NOT give if BP > 185/110 • Disability risk 30% despite ~5% symptomatic ICH risk • Lawsuits for not giving >>> lawsuits for giving
FAST TestUse the FAST test for recognizing and responding to stroke symptoms. • Facial Droop: Ask the person to smile. Does one side of the face droop? • Arm Drift: Ask the person to raise both arms. Does one arm drift downward? • Slurred Speech: Ask the person to repeat a simple sentence. Does the speech sound slurred or strange? • Time: If you observe any of these signs, it’s time to call a senior doctor.
The goal the acute management of patients with stroke is to stabilize the patient and to complete initial evaluation and assessment, including imaging and laboratory studies, within 60 minutes of patient arrival
Time Target • Door to doctor 10 min • Access to neurologic expertise 15 min • Door to CT scan completion 25 min • Door to CT scan interpretation 45 min • Door to treatment 60 min
AIS ED STROKE CARE 24/7:1-H EVALUATION, 1-H INFUSION I. Triage–10 min Review t-PA criteria Page acute stroke team Draw pre t-PA labs* II. Medical Care–25 min Place O2 , 2 NS IVs Obtain BP, weight, NIHSS Obtain 12-lead ECG Send patient to CT III. CT & Labs–45 min Obtain lab results Read CT Return pt to ED IV. Treatment–60 min Start IV t-PA Monitor for ICH sxs HTN, headache N/V, neuro status *CBC, platelets, PT/INR, PTT, chem 7, cardiac panel
Inclusion Criteria • Diagnosis of ischemic stroke causing measurable neurologic deficit • Onset of symptoms 3hours before beginning of treatment. • The patient and family understand the potential risks and benefits of therapy Recent AHA/ASA guidelines recommend extension of IV rtPA treatment window up to 4.5hours based on ECASS(III) trial
Obslute contindications • ICH (whenever the previous history) • Acute MI • Pericaditis • Endocarditis • Bleeding tendency
Exclusion Criteria • Neurologic signs are clearing spontaneously • Neurologic signs are minor and isolated • Systolic blood pressure >185 mm Hg, diastolic blood pressure >110 mm Hg • Head trauma or prior stroke in the past 3 months • MI in the last 3 months • GI/GU hemorrhage in previous 21 days • Arterial puncture at a non-compressible site during prior 7 days • Major surgery within the last 14 days
Taking any anticoagulant or if on anticoagulant INR >1.7 • Patient received heparin in the last 48 hours with elevated partial thromboplastine time (aPTT) • Platelet count of <100,000/μl • Blood glucose less than 50 mg/dl or greater than 400mg • Seizure with residual postictal focal impairments • CT scan shows evidence of multi-lobar infarction (hypo-density greater than one third of MCA territory)
Recent evidences suggest to expand the window time for the administration of rtPAfrom 3 hrs to 4.5 hrs to the above eligible patients excluding any one of the following: • *Patients older than 80 years • * All patients taking oral anticoagulants are excluded regardless of the (INR) • *Patients with baseline NIHSS greater than 25 • * Patients with a history of stroke and diabetes
No antiplatelet or anticoagulant therapy should be administered for 24 hours following tPA. Obtain a repeat head CT scan or MRI 24 hours after tPA to rule out asymptomatic hemorrhagic transformation prior to initiating antithrombotic therapy.
OTHER AIS THERAPIES:MAYBE IA, YES ASA, NO HIGH-DOSE HEPARIN • Intra-arterial t-PA • Only preliminary evidence to date, not FDA approved • Theoretical window 6 h—but do NOT preclude IV t-PA w/in 4.5 h • Studies ongoing, esp. combined w/ IV t-PA • MERCI or Penumbra device • Mechanical embolectomy devices • Theoretical window 8 h • Both FDA approved, but controlled trial results pending • Aspirin • Aspirin 325 mg per day begun within 48 h of stroke onset decreases morbidity & mortality (may begin 24 h after t-PA) • Heparin(s) • Insufficient evidence to recommend routine use of high-dose IV heparin, LMW heparin, or heparinoid as Rx for AIS per se
Penumbra Core Clot in Artery THE AIS-BP RELATIONSHIP In AIS, high BP is a response, not a cause—don’t lower it! • BP increase is due to arterial occlusion (i.e., an effort to perfuse penumbra) • Failure to recanalize (w/ or w/o thrombolytic therapy) results in high BP and poor neuro outcomes • Lowering BP starves penumbra, worsens outcomes
AIS IS NOT A HYPERTENSIVE EMERGENCY! • ASA/AHA AIS Guidelines tables no longer include recs for BP Rx in non t-PA patients • Text of guidelines state “Do not Rx unless BP > 220/120,” but also state: • No data to suggest 220/120 is dangerous & requires Rx • Evidence that BP lowering worsens outcomes is concerning • Goal is to avoid overtreating pts until definitive data available • Only definite indications to BP emergently in AIS: • AMI, CHF, Ao dissection, ARF, or HTN encephalopathy • Candidate for thrombolysis and BP > 185/110
Lower BP pre-t-PA No BP med, No t-PA MAY LOWER BP SLIGHTLY PRE T-PAMUST PICK AN UPPER LIMIT TO TREAT—220/120 IS ONE OPTION If all t-PA criteria met except sustained BP > 185/110: • Ensure 2 IVs (NS @ 75 cc/h, saline lock) • Calm patient, empty bladder • Recheck BP, lower slightly if necessary • SBP > 220 or DBP > 120 • SBP > 185 and < 220 or DBP > 110 and < 120 Avoid excessive lowering of BP just to give t-PA— “Don’t kill the penumbra to save the penumbra”
The aim is to maintain MAP = 70 - 130 mm Hg • MAP = DP + 1/3 (SP-DP) OR {(2xDP) + SP}/3 • Labetalol Initial: 20 mg IV over 2 min, then 40-80 mg IV q10min to no more than 300 • mg, OR 1-2 mg/min continuous IV infusion • Nicardipine I V: Initial 5 mg/hr slowly, may increase q15min by 2.5 mg/hr; maximum • 15 mg/h; when desired blood pressure reached, lower to 3 mg/h • Enalapril 1.25 - 5 mg IVP every 6 h • Esmolol 250 μg/kg IVP loading dose, then 25 - 300μ/kg/ min • Hydralazine 5 - 20 mg IVP every 30 min OR 1.5 to 5 μg /kg/ min • Nitroglycerin 20 - 400 μg/min • Sodium nitroprusside (0.5 mcg/kg/min)
LOWERING BP IN T-PA PATIENTS • Nicardipine 5 mg/h IV infusion • Increase 2.5 mg/h q5min to max 15 mg/h • Easily titratable without an arterial line • Labetalol 10-20 mg IV • May repeat q 10-15 min • Pre-t-PA: only use a 2nd dose only if necessary Note Different Target BPs Pre & Post T-PA Pre t-PA: < 185/110 Post t-PA: < 180/105
WORRYING ABOUT THE LUNGS:ASPIRATION, DYSPHAGIA, & OXYGEN • Weak oropharyngeal muscles common • Neurogenic dysphagia: liquids worse than solids (purees best) • Stroke pts on ventilator: 2/3 mortality, most survivors disabled • Recommendations (science): • Keep pt 100% NPO until evaluation • Use NG feeding tube if necessary (& IV NS 75-125 cc/h) • Evaluate with video fluoroscopy whenever possible • Use continuous feed only if Dobhoff tip distal to pylorus • Recommendations (art): • Maintain HOB > 30° • Maintain O2 sat > 92 or 95% w/ 2-4L O2
HYPERGLYCEMIA & ACUTE STROKE /DIABETES & 2 STROKE PREVENTION • Acutely, peri-stroke hyperglycemia associated with worse clinical outcomes • Inpatient goal BG < 150 • Chronically, each 1% in Hgb A1C results in significant in risk of death, MI, vascular complications, including 12% in stroke risk • Outpatient goal Hgb A1C < 7.0
SECONDARY STROKE PREVENTION:RISK-FACTOR MODIFICATION • Hypertension • Day 1 poststroke, start low-dose ACE-I or ARB • Slowly (days to weeks) dose, add diuretic, watch K+ • Anti-HTN meds benefit those w/ and w/o HTN history • Evaluate for sleep apnea and treat w/ CPAP • Outpatient goal < 120/80—over weeks to months *In stroke pts, ACE-Is & ARBs appear to decrease risk of stroke, MI, & vascular death beyond effect on BP alone. Based on theory and animal models, ARBs may be more effective than ACE-Is.
Vasoconstriction Na retention • Vascular proliferation Endothelial function Inflammation LDL transport ANGIOTENSIN CONVERTING ENZYME AT 1 The Bad ARB ACE-I ANGIOTENSIN I ANGIOTENSIN II Vasodilatation Natriuresis Vascular proliferation Endothelial function Apoptosis No cholesterol effect AT 2 The Good SECONDARY STROKE PREVENTION:MECHANISMS OF ACE-I/ARB BENEFITS Based on animal studies and pathophysiologic considerations, ARBs may be superior to ACE-Is for stroke prevention, but ONTARGET found no difference between telmisartan & ramipril in reducing vascular risk.
SECONDARY STROKE PREVENTION:RISK-FACTOR MODIFICATION • Hypercholesterolemia • Do not discontinue statins on admission • Obtain LDL w/in 48 of stroke onset • If LDL > 100, use hi-dose statin shown to stroke/MI/death risk • atorvastatin 20-80 mg/d • pravastatin 40-80 mg/d • simvastatin 40-80 mg/d • rosuvastatin 10-40 mg/d • If LDL < 100, use lower statin dose • Outpatient goal LDL < 70 (but give statin to all pts)
SUPPORTIVE MEDICAL CARE:PREVENT COMPLICATIONS • Aspiration (NPO until swallowing evaluation) • Deep-vein thrombosis • Sequential compression devices (if stroke < 48 h) • Heparin 5000 q8h or enoxaparin 40 mg/d • Urinary tract infection (avoid Foley catheters) • Constipation (docusate sodium for all) • Decubitus ulcers (move q2h, out of bed TID by day 2) • UGI bleed (H2B, but not cimetidine) • Fever (acetaminophen + antibiotics as indicated)
REHAB & OUTPATIENT PLANNING:BEGIN ON ADMISSION, DECREASE LENGTH OF STAY • SP—swallowing evaluation before oral feedings • PT, OT—bedside first, out of bed ASAP • Social worker—plan based on level of care, pay source, caregiver support • Communicate with primary-care clinician • Educate pt, caregiver daily (not just on discharge) • Call 911 • Follow-up after discharge • Medications • Risk Factors • Stroke Symptoms
POSTSTROKE DEPRESSION • Suspect if sxs persist 1-2 wks after stroke • Is an “organic,” not “reactive” depression • Occurs in ~ 50% of stroke pts • May affect rehab and recovery • Often resolves w/in one year • SSRIs equally effective, but if pt takes warfarin: • Escitalopram (Lexapro) 5-10 mg qAM • Citalopram (Celexa) 10-20 mg qAM • Sertraline (Zoloft) 25-50 mg qAM
OLDER PATIENTS (> 55) YOUNGER PATIENTS (< 55) Hypercoagulable states Nonatherosclerotic vasculopathies Large-artery atherosclerosis Small-artery disease Cardioembolism Hypotension Correct therapy depends on cause of stroke! “Cause” & “risk factor” are not synonymous—must Rx both! CAUSES (ETIOLOGIES) OF ISCHEMIC STROKE:SIX MAIN CATEGORIES
ETIOLOGIC EVALUATION:IDENTIFY STROKE, FIND SOURCE OF CLOT NONINVASIVE Day 1 INVASIVE Day 2 ARTERIES MRI & intracranial MRA Carotid duplex (CD) *Catheter angiogram HEART ECG & monitor Cardiac biomarkers Transthoracic echo (TTE) *TEE BLOOD *Hypercoagulable profile *in select patients
R L R L R L DWI ADC FLAIR MRI BRAIN IN HYPERACUTE ISCHEMIC STROKE • DWI & ADC: Early infarction visible • FLAIR: No signal changes; possible sulcal effacement in area of infarction
INTRACRANIAL MRA:AP VIEWS OF ANTERIOR CIRCULATION Normal Paucity of R MCA Branches c/w Embolic Occlusions RACA LACA RMCA LMCA RICA LICA RICA LICA
ECA CCA ICA Plaque CAROTID DUPLEX • Evaluates carotid arteries in neck (operable area) • Excellent screen in the right hands • May not differentiate 99 vs. 100% stenosis • Need contrast angiography for clinically relevant stenosis measurement • Carotid duplex = Doppler (velocities) + B-mode ultrasound (echo picture)
ECHOCARDIOGRAPHY:TTE VS. TEE TRANSTHORACIC ECHO Left Ventricle • Thrombus • Dilatation • SEC/smoke • Dyskinesis • Aneurysm TRANSESOPHAGEAL ECHO Left Atrium • Thrombus • Dilatation • SEC/smoke • Tumor PFO/IASA > 5 mm Endocarditis Aortic Arch • Athero > 4 mm • Thrombus • Tumor LA LV SEC/EF 20% PFO Identifies source in 37.2% of pts in NSR Identifies source in 30-40% of pts with unknown cause
CBC w/ diff & platelets PT/aPTT Fibrinogen Factor VIII Factor VII C-reactive protein Antithrombin III Protein C Protein S (total & free) Lipoprotein (a) HYPERCOAGULABLE PROFILEPATIENTS < 55 YEARS OLD • Activated protein C resistance (APCR) (& Leiden factor V mutation if APCR -) • Prothrombin G20210A mutation • Antiphospholipid antibodies • Lupus anticoagulant • Anticardiolipin abs • Anti-β-2-glycoprotein I abs • Antiphosphatidylserine abs • Methyltetrahydrofolatereductase (MTHFR) C677T & A1298C mutations • Sickle cell screen
CT / MRI APPEARANCE CANNOT DETERMINE ETIOLOGY OF SMALL CEREBRAL INFARCTS small-art. “occlusion” = small-art. “disease” • Dx of small-artery “disease” requires: • Lacunar syndrome • e.g., pure motor, pure sensory, pure sensorimotor • Medial, small (< 1.5 cm) infarct on CT or MRI • History of longstanding HTN or DM • Otherwise normal etiologic evaluation Small L subcortical infarction in 40 yo woman w/ DM—due to embolus from aortic papilloma Small-artery “disease” is a diagnosis of exclusion
SECONDARY STROKE PREVENTION:ANTITHROMBOTIC RX BASED ON CAUSE High-flow states: platelets cause clots Platelets are like Velcro sticking to bumpy walls Low-flow & hypercoagulable states: clotting factors cause clots Clotting factors are like dissolved powdered gelatin that forms clumps of Jello when liquid is static large-artery atherosclerosis small-artery disease cardioembolism hypercoagulable state ANTIPLATELET AGENT aspirin 81-325/d clopidogrel 75/d aspirin + dipyridamole XR 25/200 twice/d ANTICOAGULANT warfarin INR 2.0-3.0 or INR 2.5-3.5
SECONDARY STROKE PREVENTION:ANTIPLATELET AGENTS FOR ARTERIAL DISEASE • Aspirin • Prevents MI & stroke • Stroke rec 50-365 mg/d, but MI rec 75-162 mg/d • Low dose with less side effects, > 1200 mg/d ineffective • Enteric coating, NSAIDs may lessen efficacy • Clopidogrel 75 mg per day • Prevents MI and stroke • Routine combination with aspirin not indicated in stroke pts, though not resolved for subset of pts with large-artery athero • PPIs lessen efficacy • Aspirin / dipyridamole XR 25/200 twice daily • Data regarding MI prophylaxis lacking • Headache common side effect of dipyridamole • Not superior to clopidogrel…with more bleeding side effects
SECONDARY STROKE PREVENTION:WARFARIN FOR CARDIOEMBOLISM • Underused for a. fib./flutter, esp. blacks, Hispanics, elderly • Starting dose 5 mg qPM • INR monitoring • Target 2.5, range 2.0-3.0 (mechanical HVR 2.5-3.5) • Reflects dose 2-3 days ago, stabilizes in 10-14 days • Vitamin K (greens, NG feedings, Ensure, Slimfast, MVI) • Other meds, EtOH, cranberry juice • Dose and formulation changes • Limit holding for procedures (e.g., dental, GI, surgery)
Internal Carotid Artery D External Carotid Artery N stenosis in ICA bulb % stenosis = (D-N)/D by contrast angiography Common Carotid Artery SECONDARY STROKE PREVENTION:CAROTID STENOSIS PROCEDURES • Carotid Endarterectomy (CEA) • Clear benefit if 70-99% stenosis • Some benefit if 50-69% stenosis • Accept complication rate < 6% • Carotid Angioplasty/Stenting (CAS) • Now, option only in high-risk pts • Restenosis after CEA • Radiation-induced stenosis • Increased medical risk for CEA • Contralateral carotid occlusion • Cerebral protection devices improving, trials continue
SECONDARY STROKE PREVENTION:RISK-FACTOR MODIFICATION • Cigarette smoking cessation • Bupropion (Wellbutrin SR or XL, Zyban) • Start 150 mg daily x 3 days • Then 150 mg BID x 3 months • Nortriptyline (Pamelor) • Start 10-25 mg each night • gradually to 75 mg each night • Nicotine patch/gum/inhaler • Concurrent with bupropion or nortriptyline • Varenicline (Chantix) • Start 0.5 mg daily x 3 days • gradually to 1 mg BID x 11 wk
SECONDARY STROKE PREVENTION:RISK-FACTOR MODIFICATION • Lifestyle • Alcohol: men < 2 oz / d, women < 1 oz / d • Diet: Low saturated fat, low Na+, high K+, fruits > vegetables, Mediterranean diet • Exercise: > 20 min aerobic exercise, > 3 x / wk • Weight: maintain BMI 18.5-24.9 kg/m2 • Drugs to Avoid • Estrogen (oral contraceptives, HRT) • Sympathomimetic agents (incl. decongestants, diet pills) • NSAIDs (if taking aspirin) • PPIs (if taking Plavix)