Download
1 / 45
450 likes | 599 Views
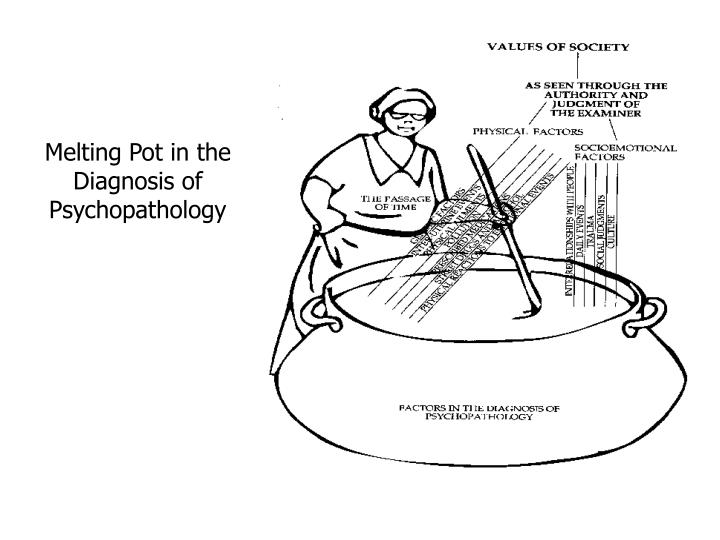
Melting Pot in the Diagnosis of Psychopathology. Mental disorder: DSV-IV.

E N D
Mental disorder: DSV-IV • A mental disorder is conceptualized as a clinically significant behavioral or psychological syndrome or pattern that occurs in an individual and that is associated with present distress (e.g. a painful symptom) or disability (I.e. impairment in one or more important areas of functioning) or with a significantly increased risk of suffering death, pain, disability or an important loss of freedom.
DSM-IV, continued • In addition, this syndrome or pattern must not be merely an expectable and culturally sanctioned response to a particular event, for example, the death of a loved one. Whatever its original cause, it must currently be considered a manifestation of a behavioral, psychological, or biological dysfunction in the individual.
DSM-IV • Neither deviant behavior (e.g. political, religious or sexual) nor conflicts that are primarily between the individual and society are mental disorders unless the deviance or conflict is a symptom of dysfunction in the individual as described above.
Problems with DSM-IV • Distress and disability do not recognize the role of outside judgment in deciding what is a disability or how serious distress has to be to become a mental disorder. • Loss of freedom could logically include all criminal behavior. • Social approbation is one sign of mental disorder--without mentioning who disapproves of whom.
Reformulated definition: A mental disorder is essentially an involuntary, organismic impairment in psychological functioning (i.e., cognitive, affective and/or behavioral). Persons who are hindered in their ability to adapt flexibly to stress, to make optimal life decisions, to fulfill desired potentials, or to sustain meaningful or satisfying relationships as a result of an impairment in cognitive, affective, and/or behavioral functioning over which they have insufficient control, have a mental disorder.
Problems with re-formulated definition • Definition includes many conditions considered by others to represent simply problems in living • This would suggest that everyone goes through life suffering from and /or tolerating a variety of mental disorders some of which are chronic (personality) • Disorder is located in the individual, does not recognize context or environment • Does not help sort out severity of illness nor ability to function.
Bases of developing a system of classification • Symptoms • many symptoms cross disorders • Behaviors • many behaviors similar among disorders • Prognosis • Frequently individualized
Bases of classification • Individual • genetics • biology (uterine environment, virus, etc) • Trauma • Interrelationships with people • Events/passage of time • Society/cultural aspects
Schizophrenia/Psychosis Mental disorder is a micro-social crisis situation in which the acts and experience of a certain person are invalidated by others for certain intelligible cultural and micro-cultural (usually familial) reasons, to the point where he/she is elected and identified as being ‘mentally ill’ in a certain way, and is then confirmed (by a specifiable but highly arbitrary labeling process) in the identity “schizophrenic patient’ by a medical or quasi-medical agents. Micro-social: a finite group of persons in face-to-face interaction. Cooper, David (1967) Psychiatry and Anti-Psychiatry Ballantine Walden, NY
How do we know mental illness? • Why do we diagnosis? • Who does it benefit? • What about the stigma? • How can we (as individuals and professionals) best support our patients?
SDV MODEL: DIATHESIS • A constitutional disposition, or predisposition, to some anomalous or morbid condition ‘which no longer belongs with the confines of normal variability, but already begins to represent a potential disease condition • Broadened: can include cognitive or social predispositions that make a person vulnerable to disorders (coping or confidence (Zubin)
SDV MODEL: Personality • The organization of traits that characterize individuals • Traits: relatively enduring dispositions of persons to react in relative consistent ways in certain kinds of situations which are prototypical for the trait.
Stress vulnerability model • Three critical factors responsible for the development of a psychiatric disorder and its course over time. These factors are interactive. • Biological vulnerability • Stress • Protective factors
Biological Vulnerability • A persons vulnerability is thought to be determined from genetic factors and early biological factors (exposure to viral infection in uterus) • The amount of vulnerability varies from one person to the next • The severity of the disorders varies also • Biological vulnerability is worsened by alcohol or drug use
Stress • The imposition of strain on a person or the effects of the strain on him; both physical and psychological factors can be stressful. Prolonged stress may impair functioning or trigger mental illness • external factor: stressor • internal: response to stress • Stress can be thought of as a response to life situations that require the individual to adapt or change. • If the person cannot adapt or change then psychiatric symptoms will appear or worsen • Stress can trigger the onset of the disorder • Stress can worsen its course • Stressors: Example of stressors include: life events, tense relationships, interpersonal difficulties (frequent arguments, strong feelings of anger or resentment in the family
Interventions based upon the stress vulnerability model of schizophrenia Stress-vulnerability-family coping skills model of adaptation to Psychiatric Disorders, Mueser & Glynn, 1990)
Risk Factors • Early childhood trauma • Sexual abuse • Physical violence • physical abuse • Parental death • Parental absences (divorce) • Parental psychopathology • Parental substance abuse
Protective factors • Protective factors reduce the person’s biological vulnerability and/or stress. • One important protective factor in schizophrenia is medication • Good coping skills in the patient and their family (such as communication or problem-solving skills) • A supportive environment can reduce stress (social support) • Providing meaningful structure
Interventions • Schizophrenia develops in a person with a biological vulnerability for the disorder which is triggered by life stress. • Protective factors such as antipsychotic medications and avoiding alcohol and substance use reduce biological vulnerability • good communication and problem-solving skills, and a supportive home environment can reduce life stress • family can support the patient to take meds, avoid substances, develop communication and problem solving, praise patient for small recovery steps and get help quickly if needed.
PTSD: normal response • PTSD normal response to abnormal situations • the incident that causes PTSD is abnormal or extraordinary • all of the reactions seen are within the limits of a normal response to such a stressor and would be expected to be seen in the majority of people experiencing the event. • Assumes that PTSD is a failure to recover from mental traumatization, however recovery is always possible. • Effects of the traumatization (all survival based): • Activation of SNS • Activation of HPA • Strong engraving of memory traces of the event • Promotion of startle response (orientation) • Heightened attention and vigilance
PTSD: abnormal alternative • PTSD is an abnormal response • symptom logy can occur after ordinary as well as extraordinary events • results from more than just event/response paradigm
Predictors of PTSD • Pretrauma Vulnerability • Magnitude of Stressor • Preparation for Event • Immediate and Short-Term Responses • Post Trauma Responses
Pretrauma vulnerability • Genetic and biological factors • Family history of mental disorders and or alcohol abuse • Gender • Neuroendocrine vulnerability (cortisol) • Personality traits (neuroticism, intr5oversion)J • Prior psychiatric disorders • Early traumatization (child abuse (sexual or physical)) • Repeated exposure to trauma • Negative parenting behavior • Early separation from parents • Parental poverty • Rearing environment (attachment)
Magnitude of stressor General characteristics: Intensity of traumatic event Duration of traumatic event Frequency of traumatic event Dangerousness of event (perceived threat to existence) 7 genetic dimensions of traumatic stress 1. Threat to one’s life and body integrity 2. Severe physical harm or injury 3. Receipt of intentional injury/harm 4. Exposure to the grotesque 5. Witnessing or learning of violence to loved ones 6. Learning of exposure to a noxious agent 7. Causing death or severe harm to another
Preparation for the Event • “IF POSSIBLE” • . . . . adequate preparation for a stressful event helps protect individuals from the effect of stress
Immediate or short-term responses • Peritraumatic responses: • Observable behavior of symptoms • Conversion, agitation or stupor • Emotional or cognitive experience • Anxiety, panic, numbing confusion • Mental processes • Psych. Defenses • Dissociation, • freezing/surrender and or disorganization and the perception of events as uncontrollable or unpredictable have long-term effects
Immediate or short-term responses • All coping efforts seem to have same effect (lessening impact), what is important is that person feels they have some ability to cope. • Survivors of terrorist attack: (Israel) • Actively rescuing other survivors • Sharing important information with the rescuers • Preserving one’s dignity by covering one’s body • Controlling the disclosure of information about the event to one’s relatives
Post trauma responses • Intrusive symptoms • 48 hours after the event • For many the repeated memories are intolerable • Survivors may be judging themselves and reevaluating their actions • The reevaluating may lead to the formation of negative beliefs about oneself and others • PTSD and rape victims (Rothbaum, 1989) • 94% had symptoms of PTSD within 1 week of trauma • 52% - 2 months later • 47% - 9 months later • Serin Gas release in Tokyo subway • Seen for first two year-no signs of PTSD • PTSD symptoms appeared 5 to 6 years after the event in over 50% of people exposed.
Children and trauma • Children exposed to early adverse experiences are at increased risk for the development of depression or anxiety disorders • 1.5 million verified cases of child maltreatment reported annually in US • A large number of children experience the loss of a parent • A large number of children live with a mentally ill parent unable to provide continuous parental care
Mental disorders and childhood • Relationship between disorganized attachment and psychopathology in childhood • Increase in ADHD, behavior problems, social problems, Oppositional Defiant disorder in boys, difficult temperament (predictor of aggressive behavior), cognitive immaturity
Resilience • GxE-study team-Kings College, London • Work of Sir Michael Rutter • Terrie Moffitt • Avshalom Caspi • Stems from the work of: • Norman Garmezy (1960’s) and Ann Masten (1970’s) at University of Minnesota
Resilience • Resilience-springing back from serious adversity. • highly subjective definition • Reviewing the literature of the long term effect of physical and/or sexual child abuse, 20 to 40% of the maltreated children show few signs of behavioral or mental health problems in later life. • Why are some people able to experience extreme adversity and yet lead successful/satisfying lives?
GxE • Interplay between particular genes and environment. • A particular variant of a gene can promote resilience and perhaps buffer against the ruinous effects of adversity. • In the absence of the aversive environment the gene does not express itself.
5-HHT Promotor Gene • 5-HHT gene is critical for regulation of serotonin in brain. • 5-HHT gene has two alleles and each allele occurs in either a short or a long version. • People with at least one Short allele are more prone to depression. Moffitt and Capsi-Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene Science, vol: 301, July, 2003.
Types of variation • 33% of (US-white population) have two copies of the protective long allele. • 50% have one long allele and one short allele • 17% have two short alleles • (africian-americans are less likely to have short allele, Asians are more likely)
Prospective study of 847 adults • Found link (correlation) among having at least one short 5-HHT allele and elevated rates of depression in adults who had experience mistreatment as children or significant stress/adversity.(moderate risk) • Having two short 5-HHT alleles increased the likelihood of depression as an adult. • Two long alleles the link was low for subsequent depression.
Conclusions • In other words: • “children with two risky alleles lost out badly when their environments failed them, children with one risky allele were at some increase (sic) risk and children with good resilience alleles (two long, sic) carried a shield. “ • Emily Baxelon, New York Times, April 30th, 2006.
Stephen Suomi, NIMH • Two groups of monkeys (rhesus). • One group raised by Mom in Laboratory but similar to “wild” experience. • Second group created to mimic experience of a neglected or abused child. Never see mother, spend two weeks in an incubator and then moving into small groups of peers. • Rhesus monkeys hare 96% of their genes in common with humans, including the long and short variations of 5-HHT. • Monkeys are DNA tested and one short/long and two long monkeys can be categorized. Shannon C, Schwandt ML, Champoux M, Shoaf SE, Suomi SJ, Linnoila M, Higley JD. Maternal absence and stability of individual differences in CSF 5-HIAA concentrations in rhesus monkey infants. AM J Psychiatry. 2005 Sep;162(9):1658-64. Christina S. Barr, Timothy K. Newman, Melanie Schwandt, Courtney Shannon, Rachel L. Dvoskin, Stephen G. Lindell, Julie Taubman,§ Bill Thompson,¶ Maribeth Champoux, Klaus Peter Lesch, David Goldman, Stephen J. Suomi,and J. Dee Higley. Sexual dichotomy of an interaction between early adversity and the serotonin transporter gene promoter variant in rhesus macaques. Proc Natl Acad Sci U S A. 2004 August 17; 101(33): 12358–12363.
Findings • In motherless, peer raised monkeys who have one short/long pairs 5-HHT alleles are more likely to experience fear, panic, aggression (low serotonin acid in CSF) when a strange monkey in placed in a cage next to them. • motherless, peer raised monkeys who have a 2 long 5-HHT alleles are more likely to take the presence of the stranger monkey in stride (similar to mother raised monkeys). • (since it is rare to find a rhesus monkey with two short alleles for 5-HHT their conditions was not tested.
Conclusions • Findings are similar to Australian study by Moffitt/Caspi. • Suomi: “How you grow up affects your hormonal output and the structure and function of the brain. And these effects are tempered by the kind of gene the monkeys carry, so it is a true interaction?
Behavioral description The group is in a caged together, mother raised and non-mother raised. When people walk in (even Suomi who goes in daily) some of the monkeys stay in the middle of the cages and ignore the stranger. Another group races to the back of the cage and huddles together in the farthest corner their small fingers wrapping around one another’s fur. They twitter and turn their faces away in distress. Middle of the cage monkeys were mother raised, the ones at the back were motherless. After a few minutes some of the peer raised monkeys begin to dart forward to peers, and after a few more minutes they settle in with the mother-raised group. But others never move from the back. The monkeys who raced to the back but eventually came forward and mirror human resilience were the monkeys with two long 5-HHT alleles. • Emily Brazelon