Download
1 / 17
170 likes | 355 Views
HEAD AND NECK: hn 17. ETHMOIDO-SPHENO-ORBITAL FIBROUS DYSPLASIA: A REPORT CASE. L. EL ASSASSE, S. BOUTACHALI, T. AMIL, A. HANINE, S. CHAOUIR, A. DARBI. Radiology service, Military hospital, Rabat, Morocco. Introduction:.

E N D
ETHMOIDO-SPHENO-ORBITAL FIBROUS DYSPLASIA: A REPORT CASE L. EL ASSASSE, S. BOUTACHALI, T. AMIL, A. HANINE, S. CHAOUIR, A. DARBI. Radiology service, Military hospital, Rabat, Morocco
Introduction: • Fibrous dysplasia is an uncommon bone disease in young patients, characterized by defective bone maturation localized in one or more bone sites. • The craniofacial involvement represents 20% of all locations. • We present in this work the case of an ethmoido-spheno-orbital location.
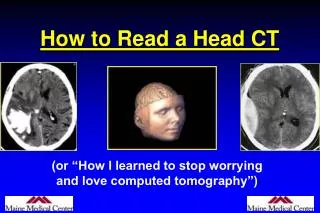
Observation: • A 6 year old girl without particular history presented right painless exophthalmia associated with ipsilateral hemi-cranial headache. • Craniofacial CT shows an expansive right ethmoid process with extension into the sphenoid sinus and right orbit. • Treatment consisted of surgical resection. • Histological examination confirmed the diagnosis of fibrous dysplasia.
Craniofacial CT (bone windows) shows an expansive right ethmoid process with extension into the sphenoid sinus and right orbit.
Discussion: • Fibrous dysplasia was first described by Lichtenstein in1938 as a disorder characterized by progressive replacement of normal bone elements by fibrous tissue. • It is a bone tumor that, although benign, has the potential to cause significant cosmetic and functional disturbance, particularly in the craniofacial skeleton. • Its management poses significant challenges to the surgeon. Its compression of the optic nerve with resulting visual impairment is especially alarming.
Discussion: • Over the years, we have gained a better understanding of its etiology, clinical behavior, and both surgical and non-surgical treatments. • Its characteristics, under various imaging modalities, have been thoroughly described in recent years.
Discussion: • Fibrous dysplasia is a benign disease which often affects subjects between 10 and 30 years. • It may be monostotic or polyostotic, isolated or within the context of McCune-Albright syndrome. • The discovery of this pseudotumor may be fortuitous or further to deformation and clinical manifestations of the nervous compression which it can engender.
Discussion: • The plain radiological features of FD are non-specific and vary widely. The typical appearance is that of radiolucent lytic lesions with a homogenous ground-glass appearance and illdefined borders. Occasionally, the radiograph may reveal predominantly sclerotic lesions with or without accompanying lytic lesions. • Naturally, its nonspecific radiological appearance makes it difficult to differentiate from other conditions such as ossifying fibroma and Paget’s disease.
Discussion: • Computed tomography (CT) is a better radiological tool, especially for assessing the extent of the tumor in cases of suspected optic canal involvement. While it is invaluable in pre-operative planning, it is also a superior diagnostic tool, although CT alone is insufficient to make a diagnosis of FD. • FD has characteristic appearances on CT and consists of three varieties: ground-glass pattern (56%), homogeneously dense pattern (23%) and cystic variety (21%).
Discussion: • Various studies have suggested the use of magnetic resonance imaging (MRI) as a diagnostic tool for FD. Lesions have been characterized by a decreased signal as well as sharply demarcated borders on both T1- and T2-weighted images. • Some authors, however, have highlighted the potential for misdiagnosis with MRI. The MRI characteristics of FD do not share the distinctive features seen on radiography or CT, and often resemble that of tumors.
Discussion: • This is particularly so when the lesion shows intermediate signal intensities on T1-weighted images and high signal intensities on T2-weighted images, and enhances brilliantly after the injection of contrast material. • The likelihood of correctly diagnosing FD by MRI is high only when the signal intensities on both T1- and T2-weighted images are low in spite of the injection of contrast material.
Discussion: • Radionuclide scans, such as bone scintigraphy, have some role in the diagnosis/evaluation of FD. • Radionuclide scan has high sensitivity but low specificity. • Single photon emission computed tomography (SPECT) has been reported to be more sensitive in detecting the areas involved in cases of FD.
Discussion: • Treatment ranges from therapeutic abstention and mutilating surgery.
Conclusion: • The diagnosis of fibrous dysplasia is mainly based on CT which shows a characteristic frosted glass, and allows to draw an accurate mapping of the lesions and to determine the degree of impact on the anatomical elements of the neighborhood. • But diagnosis of certainty remains histological.
REFERENCES: 1-Rahman AMA, Madge SN, Billing K, Anderson PJ, Leibovitch I, Selva D, David D. Craniofacial fibrous dysplasia: clinical characteristics and long-term outcomes. Eye 2009; 23: 2175-81. 2-Feller L, Wood NH, Khammissa RAG, Lemmer J, Raubenheimer EJ. The nature of fibrous dysplasia. Head & Face medicine 2009;Vol 5: 22. 3-Chen YR, ChangCN, Tan YC. Craniofacial fibrous dysplasia: An update. Chang Gung Med J 2006; 29: 543-9. 4- Ziadi S, Trimecho M, Mokni M, Sriha B, Khochtali H, Korbi S. Dix-huit cas de dysplasie fibreuse cranio-faciale. Rev Stomatol Chir Maxillofac 2009; 110: 318-22.
REFERENCES: 5-Loeb I, Boutremans E. La dysplasie fibreuse. Rev Stomatol Chir Maxillofac 2005; 106; 5: 311-2. 6-Arkha Y, Benazzou S, Harmouch A, Derraz S, El Ouahabi A, El Khamlichi A. Un cas de dysplasie fibreuse kystique cranio-faciale. Rev Stomatol Chir Maxillofac 2010; 111: 101-4.