Download
1 / 81
820 likes | 1.12k Views
LUNG PATHOLOGY. Review Of Anatomy & physiology. Cartilage is present to level of proximal bronchioles Beyond terminal bronchiole gas exchange occurs The distal airspaces are kept open by elastic tension in alveolar walls. Pulmonary Atelectasis. Pulmonary Atelectasis. Lung Collapse

E N D
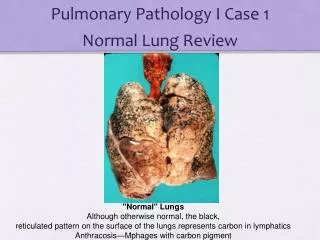
Review Of Anatomy & physiology • Cartilage is present to level of proximal bronchioles • Beyond terminal bronchiole gas exchange occurs • The distal airspaces are kept open by elastic tension in alveolar walls
Pulmonary Atelectasis • Lung Collapse • loss of lung volume caused by inadequate expansion of airspaces • May involve the entire lung, a lobe or a segment
ARDS (Diffuse alveolar damage
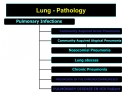
Asthma Asthma is a chronic inflammatory disorder of the airways that causes recurrent episodes of wheezing, breathlessness, chest tightness, and cough, particularly at night and/or in the early morning. These symptoms are usually associated with widespread but variable bronchoconstriction and airflow limitation that is at least partly reversible, either spontaneously or with treatment.
These lungs appear essentially normal, but are normal-appearing because they are the hyperinflated lungs of a patient who died with status asthmaticus.
The cut section of the hyperinflated lung of a patient dying in status asthmaticus appears essentially normal.
What are the 4 classical histologic findings in bronchial asthma?
This cast of the bronchial tree is formed of inspissated mucus and was coughed up by a patient during an asthmatic attack. The outpouring of mucus from hypertrophied bronchial submucosal glands, the bronchoconstriction, and dehydration all contribute to the formation of mucus plugs that can block airways in asthmatic patients.
Between the bronchial cartilage at the right and the bronchial lumen filled with mucus at the left is a submucosa widened by smooth muscle hypertrophy and inflammation (mainly eosinophils). These are changes of bronchial asthma. The peripheral eosinophil count or the sputum eosinophils can be increased during an asthmatic attack.
At high magnification, the numerous eosinophils are prominent from their bright red cytoplasmic granules in this case of bronchial asthma.
Bronchiectasis • Is the permanent dilation of bronchi and bronchioles caused by destruction of the muscle and elastic supporting tissue
This is another form of obstructive lung disease known as bronchiectasis. Bronchiectasis occurs when there is obstruction or infection with inflammation and destruction of bronchi so that there is permanent dilation. Once the dilated bronchi are present, as seen here grossly in the mid lower portion of the lung, the patient has recurrent infections because of the stasis in these airways. Copius purulent sputum production with cough is typical.
A closer view demonstrates the focal area of dilated bronchi with bronchiectasis. Bronchiectasis tends to be localized with disease processes such as neoplasms and aspirated foreign bodies that block a portion of the airways. Widespread bronchiectasis is typical for patients with cystic fibrosis who have recurrent infections and obstruction of airways by mucus throughout the lungs.
Bronchiectasis is seen here. The repeated episodes of inflammation can result in scarring, which has resulted in fibrous adhesions between the lobes. Fibrous pleural adhesions are common in persons who have had past episodes of inflammation of the lung that involve the pleura. With extensive involvement, the pleural space may be obliterated.
The mid lower portion of this photomicrograph demonstrates a dilated bronchus in which the mucosa and wall is not clearly seen because of the necrotizing inflammation with destruction. This is the microscopic appearance of bronchiectasis. Bronchiectasis is not a specific disease, but a consequence of another disease process that destroys airways.
Chronic Bronchitis Chronic productive cough on most days of 3 consecutive months in 2 consecutive years Providing other causes have been excluded.. The pathological hallmarks of chronic bronchitis are congestion of the bronchial mucosa and a prominent increase in the number and size of the bronchial mucus glands.
Chronic bronchitis does not have characteristic pathologic findings, but is defined clinically as a persistent productive cough for at least three consecutive months in at least two consecutive years. Most patients are smokers. Often, there are features of emphysema as well.
Emphysema Abnormal and permanent dilatation of air spaces associated with destruction of their walls.
The chest cavity is opened at autopsy to reveal numerous large bullae apparent on the surface of the lungs in a patient dying with emphysema. Bullae are large dilated airspaces that bulge out from beneath the pleura. Emphysema is characterized by a loss of lung parenchyma by destruction of alveoli so that there is permanent dilation of airspaces.
On cut section of the lung, the dilated airspaces with emphysema are seen. Although there tends to be some scarring with time because of superimposed infections, the emphysematous process is one of loss of lung parenchyma, not fibrosis.
CENTRI-acinar PAN-acinar
Microscopically at high magnification, the loss of alveolar walls with emphysema is demonstrated. Remaining airspaces are dilated.
Here is the gross appearance of a lung with tuberculosis. Scattered tan granulomas are present, mostly in the upper lung fields. Some of the larger granulomas have central caseation. Granulomatous disease of the lung grossly appears as irregularly sized rounded nodules that are firm and tan. Larger nodules may have central necrosis known as caseation
This is another example of granulomatous disease of the lung. The pattern of smaller nodules which have a propensity for upper lobe involvement suggests a granulomatous process rather than metastatic disease.
On closer inspection, the granulomas have areas of caseous necrosis. This is very extensive granulomatous disease. This pattern of multiple caseating granulomas primarily in the upper lobes is most characteristic of secondary (reactivation) tuberculosis.
When there is extensive caseation and the granulomas involve a larger bronchus, it is possible for much of the soft, necrotic center to drain out and leave behind a cavity. Cavitation is typical for large granulomas with tuberculosis.
There is a small tan-yellow subpleural granuloma in the mid-lung field on the right. In the hilum is a small yellow tan granuloma in a hilar lymph node next to a bronchus. This is the "Ghon complex" that is the characteristic gross appearance with primary tuberculosis.
The Ghon complex is seen here at closer range. Primary tuberculosis is the pattern seen with initial infection with tuberculosis in children. Reactivation, or secondary tuberculosis, is more typically seen in adults.
Well-defined granulomas are seen here. They have rounded outlines. The one toward the center of the photograph contains Langhans giant cells. Granulomas are composed of transformed macrophages called epithelioid cells along with lymphocytes, occasional PMN's, plasma cells, and fibroblasts. The localized, small appearance of these granulomas suggests that the immune response is fairly good.
At low magnification, this photomicrograph reveals multiple granulomas. Granulomatous disease by chest radiograph can appear as reticulonodular densities.
The edge of a granuloma is shown here at high magnification. At the upper right is amorphous pink caseous material composed of the necrotic elements of the granuloma as well as the infectious organisms. This area is ringed by the inflammatory component with epithelioid cells, lymphocytes, and fibroblasts.
At high magnification, the granuloma demonstrates that the epithelioid macrophages are elongated with long, pale nuclei and pink cytoplasm. The macrophages organize into committees called giant cells. The typical giant cell for infectious granulomas is called a Langhans giant cell and has the nuclei lined up along one edge of the cell.
In order to find the mycobacteria in a tissue section, a stain for acid fast bacilli is done (AFB stain). The mycobacteria stain as red rods.
When the immune response is poor or is overwhelmed by an extensive infection, then it is possible to see the gross pattern of granulomatous disease seen here. This is a "miliary" pattern of granulomas because there are a multitude of small tan granulomas, about 2 to 4 mm in size, scattered throughout the lung parenchyma. The miliary pattern gets its name from the resemblence of the granulomas to millet seeds.