Download
1 / 37
480 likes | 832 Views
For more presentations and information visit http://www.pharmaxchange.info. DIRECT FACTOR Xa INHIBITOR AS ANTICOAGULANT. PREET PAL SINGH SIDHU DEPT OF MEDICINAL CHEMISTRY SCHOOL OF PHARMACY, VCU. OVERVIEW. For more presentations and information visit http://www.pharmaxchange.info.

E N D
For more presentations and information visit http://www.pharmaxchange.info DIRECT FACTOR Xa INHIBITOR AS ANTICOAGULANT PREET PAL SINGH SIDHU DEPT OF MEDICINAL CHEMISTRY SCHOOL OF PHARMACY, VCU.
OVERVIEW For more presentations and information visit http://www.pharmaxchange.info • Introduction • Comparison with current therapy. • Natural inhibitors of Factor Xa. • Structural details of active site. • Trend in Factor Xa inhibitors. • Rivaroxaban • - SAR • - Synthesis • - Crystal structure • - pharmacokinetic profile • 7. Apixaban • - Synthesis • - Crystal structure • - Pharmacokinetic profile • 8. Conclusion.
INTRODUCTION For more presentations and information visit http://www.pharmaxchange.info • Factor Xa is K-dependent serine protease. • Molecular Wt is 45 K. • Factor Xa occupies the pivotial position in coagulation cascade. • Factor X is zymogen of Factor Xa. • Circulates in plasma as a light- and heavy-chain held together by a disulfide bond. • N-terminal light chain contain GLA and two epidermal growth factor-like domain. • C-terminal heavy chain contain the trypsin-like catalytic domain. • First Factor Xa deficiency was described in 1950s.
INTRODUCTION For more presentations and information visit http://www.pharmaxchange.info Two physiological inhibitor: 1)Tissue factor pathway inhibitor: Regulate inhibition by Fxa dependent inhibition of FVIIa-Tissue factor complex during initial stage. Function by binding the active site of Fxa and FVIIa-Tissue factor Via second and first kunitz domain. No co-factor requirement. 2)Antithrombin: Serine protease type inhibitor. Function by binding site of Fxa through exposed reactive center loop and induces the conformational change which trap enzyme in inactive, stable complex. Require co-factor ( Glycosaminoglycans). Rezaie et al, biochemistry, 2002, 41, 6780
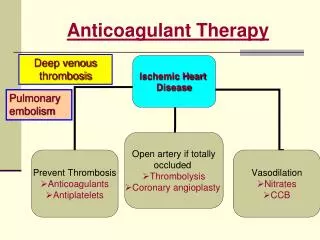
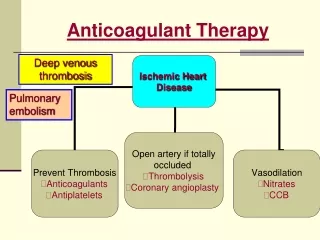
MECHANISM For more presentations and information visit http://www.pharmaxchange.info EXTRINSIC PATHWAY FACTOR Xa INTRINSIC PATHWAY PHOSPHOLIPID FVa-Fxa Ca+ Direct Factor Xa inhibitor Prothrombinase complex Prothrombin thrombin platelet aggregation fibrinogen fibrin clot FXa
DISADVANTAGES OF CURRENT THERAPY For more presentations and information visit http://www.pharmaxchange.info General disadvantage of current therapy: Slow onset of action parenteral mode of administration excessive bleeding Stringent monitoring requirement HEPARIN: Parenteral administration. Monitoring requirement. Excessive bleeding. WARFARIN: Excessive bleeding. Monitoring requirement. Severe enzyme induction. Advantages: Low cost, Fast onset of action Advantage: Oral dose
PREFERREDPROFILE For more presentations and information visit http://www.pharmaxchange.info • A wide therapeutic window of antithrombotic effect versus bleeding. • A rapid onset and offset of action. • Oral bioavailability • No coagulation monitoring required. • Inhibition of free and clot- bound thrombin. • Reproducible PK and PD profile. • Minimal interaction with food and other drugs. • Minimal dose frequency. Weitz et al blood 2005 105 453 Hirish et al thromb res 2003 9 suppl 1:S1-8
COMPARISON OF ANTICOAGULANT For more presentations and information visit http://www.pharmaxchange.info
NATURAL INHIBITORS For more presentations and information visit http://www.pharmaxchange.info Antistasis- • Isolated from extracts of mexican leech in 1987. • It is slow, tight binding, selective Factor Xa inhibitor. • Ki=0.3-0.6 nM. TAP- • A single 60 amino acid peptide isolated from extract of tick. • Reversible, slow, tight binding inhibitor of Factor Xa. • Ki=0.5 nM. Ghilanten- • Isolated from south American leech. Simpson et al, j. biol. Chem, 1989, 264, 16694 Waxman et al, science,1990, 248, 593
S1 POCKET For more presentations and information visit http://www.pharmaxchange.info Most important pocket for binding for substrate or inhibitor. Formed by 214-220 and 189-195 loops tied together by CYS 220- CYS 191 Disulfide bond. Residues 225-228 form the base and lower strand of pocket. Important residues are ASP 189, ALA 190 and GLN 192. Rai et al current med chem, 2001, 8,101
S2 POCKET For more presentations and information visit http://www.pharmaxchange.info A small pocket merged with S4 pocket. Likely this pocket defines the selectivity of selective Factor Xa inhibitor over thrombin. Rai et al current med chem, 2001, 8,101
S3 POCKET For more presentations and information visit http://www.pharmaxchange.info Located on the rim of S1 pocket. Most of Factor Xa inhibitor do not interact with this region. Rai et al current med chem, 2001, 8,101
S4 POCKET For more presentations and information visit http://www.pharmaxchange.info S4 and S1 pocket represent the important binding region. It is large and well defined pocket. S4 pocket the 3 sub-regions: Hydrophobic box Cationic hole water site Hydrophobic box composed of Phe 174, Tyr 99, Trp 215. Cationic hole is formed by Glu97 and Lys96. Water is trapped underneath the Thr98, Ile175, thr175. Rai et al current med chem, 2001, 8,101
TREND IN Fxa INHIBITORS For more presentations and information visit http://www.pharmaxchange.info Factor Xa inhibitors can be divided into three fragments: P1 Group: Binds in the S1 sub-pocket. Central Scaffold: project the substituent's into sub-pocket. P4 Group: Binds in the S4 sub-pocket. P1 group is further divided into 3 types: - Highly Basic Group. - Moderately Basic Group. - Neutral Group. Scaffold is further divided into 2 types: - Flexible Scaffold. - Rigid Scaffold. Maignan et al. Curr. Top. Med. Chem. 2001, 1, 161
HIGHLY BASIC P1 GROUPS For more presentations and information visit http://www.pharmaxchange.info • -salt bridge with Asp189 • H-bond with Gly219 • Poor bioavailability • 10 fold increased potency • -Enhanced oral absorption Benzamidine Napthyl amidine -Similar inhibition constant -Enhanced oral absorption -4-fold more active than benzamide series Amidino thiophene Amidino indole
MODERATELY BASIC P1 GROUPS For more presentations and information visit http://www.pharmaxchange.info Form water mediated interaction with Asp189 Form H- bond with Gly219 10 times better at crossing Caco-2 monolayer than benzamidine Amino isoquinolines Similar pharmacokinetic activity and binding mode as amino isoquinolines Aza indole
NEUTRAL P1 GROUP For more presentations and information visit http://www.pharmaxchange.info -Introduced by Lilly pharm. -17-fold lower inhibition -Improved Pk profile -6-fold increase in potency -Efficacy same as benzamidine Chloro phenyl Methoxy benzoyl Chloro thiophene Chlorothiophene
LINKER SCAFFOLDS (FLEXIBLE) For more presentations and information visit http://www.pharmaxchange.info Aliphatic chain Amide bond Amide ester - To remove chiral center - Gain H-bond to Gly219 - By Daiichi Pharm. • By Aventis Pharm. • Increases potency by 9 fold • Increases selectivity by 5 fold • Ester group located in small hydrophobic pocket Allyl linker Sulfonamide Pentanoic acid -Designed to circumvent chiral center
LINKER SCAFFOLDS (RIGID) For more presentations and information visit http://www.pharmaxchange.info Sulfonamido pyrrolidinone Ether link Cyclo heptanonediene Cyclic urea By Aventis pharm. Potential for additional interaction. By Berlex. Photochemical liable By Berlex Optimal linker By DuPont H- bond with Gly216 Benzimidazole Carbazole Benzoxazinone By Berlex To add hydrophilicity Introduced by Pfizer By Berlex To add hydrophilicity
P4 GROUPS For more presentations and information visit http://www.pharmaxchange.info Methoxy benzene Amido diphenyl By Lilly Pharm. Phenyl lies parallel to Trp215 mM potency Phenyl sulfonamide Additional H-bond with Gly219 Pyridyl piperidine By DuPont Pharm. Edge to face with Trp215 OH interact with Tyr99 To increase hydrophilicity Pyridine stack with Trp215 H-bond with structural water Benzyl sulfonyl piperidine Amido benzofuran Methoxy naphthalene sulfonamide Phenyl imidazoline Sulfonamide has conformational role Edge to face interaction with Trp215 Piperidine play no role Parallel to Trp215 By Berlex Both ring are parallel to each other and perpendicular to Trp215 H-bond with Asn97
DRUGS AND THEIR CURRENT STATUS: For more presentations and information visit http://www.pharmaxchange.info
RIVAROXABAN(BAY-59-7939) For more presentations and information visit http://www.pharmaxchange.info • Oral , direct Fxa inhibitor under development. • It is oxazolidinone derivative. • IC50=21nM. • Currently in Phase III of clinical trail. • If approved , it will be marked by name Xarelto. • It is joined product of Bayer and ortho-McNiel pharmaceuticals.
SAR OF RIVAROXABAN For more presentations and information visit http://www.pharmaxchange.info 1 IC50= 120nM 2 IC50= 8nM 3 IC50= 20μM 4 IC50= 90nM
SAR OF RIVAROXABAN For more presentations and information visit http://www.pharmaxchange.info Roehrig S, Straub A, Pohlmann J, et al. J. Med. Chem.48 (19): 5900
SAR around the aryl moiety For more presentations and information visit http://www.pharmaxchange.info R1 R2 R3 ent IC50 [nM] H , H s 4.0 H , H s 0.7 F , H s 1.4 CF3, H s 1.O NH2, H s 2.5 H , CH3 s 1260 H , H R 2300 R1 R2 R3 ent IC50 [nM] F , H s 90 F , H s 32 H , H s 43 F , H s 40 H , H s 74 F , H s 140
Modifications on the amide linker and thiophene moiety R1 X R2 IC50 [Nm] CO H 2000 CO H 8.5 CO H 290 CO H 29 CO H 94 CO CH3 197 SO2 H 1200 R1 X R2 IC50 [Nm] CO H 0.7 CO H 0.4 CO H 9.2 CO H 26 CO H 20 CO H 1170 For more presentations and information visit http://www.pharmaxchange.info
SYNTHESIS OF RIVAROXABAN (SCHEME I) For more presentations and information visit http://www.pharmaxchange.info Bayer healthcare Drug Fut 2006, 31, 484
SYNTHESIS OF RIVAROXABAN (SCHEME I) For more presentations and information visit http://www.pharmaxchange.info Bayer healthcare Drug Fut 2006, 31, 484
SYNTHESIS OF RIVAROXABAN (SCHEME II) For more presentations and information visit http://www.pharmaxchange.info Bayer healthcare Drug Fut 2006, 31, 484
CRYSTAL STRUCTURE For more presentations and information visit http://www.pharmaxchange.info MAJOR BINDING COMPONENT 1. Hydrogen with Gly219 2. L-Shape provided by oxazolidine 3. Carbonyl doesn’t interact 4. Chlorine-Tyr228 interaction Bayer healthcare, J. Med. Chem, 2005, 48, 5900
PHARMACOKINETIC PROFILE For more presentations and information visit http://www.pharmaxchange.info ABSORPTION AND DISTRIBUTION: Peak plasma conc. is reached in 2 to 4 hours after oral administration. Bioavailability range from 60-80%. Presence of food increases maximum conc., time to maximum conc. and AUC. Bound extensively to protein (90%). No effect of increased gastric pH on PK-PD profile. METABOLISM: Hepatic metabolism Via cytochrome P-450 3A4. EXCRETION: Both renal and hepatic excretion. 36% of drug is excreted unchanged in urine.
PHARMACOKINETIC PROFILE For more presentations and information visit http://www.pharmaxchange.info EFFECT OF AGE: AUC was higher in patient above 75 years. EFFECT OF RENAL INSUFFICIENCY: AUC was 44%, 52%, 64% higher in mild, moderate and severe renal insufficiency. Still no recommendation in dose adjustment for renal insufficiency. EFFECT OF HEPATIC INSUFFICIENCY: With mild hepatic disease, no difference in PK-PD profile. With moderate hepatic insufficiency, decrease in total body clearance. Patient with severe renal failure are excluded from clinical trails. EFFECT OF OBESITY: Compared in different weight group (<50, 50-80, 80-120, >120). In higher Wt. group, AUC and inhibition was lower. In lower Wt. group, Cmax was higher and half life was 2 hour longer. EFFECT OF GENDER AND RACE: No difference in PK-PD was found between the gender.
APIXABAN For more presentations and information visit http://www.pharmaxchange.info Apixaban is follow-up compound of razaxaban, a direct Fxa inhibitor. Highly selective and potent (Ki=0.8nM) inhibitor of both free and bound Fxa. It is product of Bristol-Myers Squibb (BMS). CURRENT STATUS: 1). Phase III for VTE prevention study. 2). Phase III for prevention of stroke. 3). Phase III for other thromboembolic events in patient with atrial fibrillation.
SYNTHESIS OF APIXABAN For more presentations and information visit http://www.pharmaxchange.info 4 2 1 3 5 6
CRYSTAL STRUCTURE For more presentations and information visit http://www.pharmaxchange.info
PHARMACOKINETIC PROFILE For more presentations and information visit http://www.pharmaxchange.info ABSORPTION AND DISTRIBUTION: Apixaban is rapidly absorbed, Cmax in 1 hour. Oral bioavailability is 80%. Average half life is 12 hours. METABOLISM: 70% of drug excreted unchanged. CYP3A4 may be involved in metabolism. EXCRETION: 60% excreted by fecal route. 25% excreted in urine. Minor route of excretion is biliary. Zhang et al, Drug. Met. Disp. 2008 (in press)
DO FACTOR Xa RELATE WITH CANCER?? For more presentations and information visit http://www.pharmaxchange.info • Cancer patient have elevated level of coagulation abnormalities. • Thrombosis is most frequent complication and 2nd leading cause of death in cancer. • Factor Xa, thrombin and tissue factor contribute to tumor growth. • Factor Xa promote tumor growth in 2 ways: • Fibrin provide network for growth and block access of immune system. • Recognition and binding to tumor cell to initiate cellular event. • Heparin suppress small cell lung cancer and B16 melanoma cell growth in animals. • Antistasin suppress T241 sarcoma cell growth in mice. • Ghilanten also suppress B16 melanoma cell growth in mice. • DX-9065a shown to inhibit A549 lung adenocarcinoma cell proliferation.