Download
1 / 34
340 likes | 459 Views
Cancer Mapping: Making Spatial Models Work for Communities. CEHTP-TIAG Meeting Oakland, CA March 21, 2012. Agenda. Motivations for project Advisory Group (AG) process Protocol development Analytic results from AG-led protocol. Context.

E N D
Cancer Mapping: Making Spatial Models Work for Communities CEHTP-TIAG Meeting Oakland, CA March 21, 2012
Agenda • Motivations for project • Advisory Group (AG) process • Protocol development • Analytic results from AG-led protocol
Context • Public health agencies receive 1,000 – 2,000 inquiries per year about local-scale cancer rates • Often referred to as “cluster inquiries” • Routinely generated information almost universally confined to county-level rates • Many approaches available for calculation of statistically reliable, confidentiality-protecting rates below the county level • Public health agencies often uninterested and/or unable to choose among these approaches • Might an experienced, well-informed group of cancer advocates be able to provide this leadership?
Project overview • 2 year grant funded by CA Breast Cancer Research Program (CBCRP) • Overall questions: • Should mapping of breast cancer at the census tract level be conducted? • How? Why? • Year 1 (Sep. 2009-Aug. 2010) • Outreach and recruitment for Advisory Group (AG) • Methods review • Selection of methods by Advisory Group • Year 2 (Sep. 2010-Aug. 2011) • Apply preferred methods to actual CCR data • Present findings to Advisory Group • Outline communication strategy • Develop and disseminate final product
Necessary Discussions • What do we mean by “cancer mapping?” • What would cancer maps tell us? What would they not tell us? • What actions could and/or should be taken based on likely information? • Is there a “best practice” for cancer mapping? • What are the responsibilities of public agencies? Of communities? • On balance, is census tract-level cancer mapping even a good idea?
Strategies • Establishment of common language so participants having diverse backgrounds can work as a group • Use of visual, interactive examples to facilitate discussion of abstract concepts • Maps of hypothetical communities • Hypothetical “cluster” findings • Performance of various analytic techniques under different circumstances (“What we would get if we chose this…”)
What difference does each method make? • Sensitivity, specificity, false positive rate, true positive rate; these depend on: • The disease (in this case, invasive breast cancer) • Choice of cut point (e.g. “p< 0.05”) • Focusing on technical terminology would not: • Be helpful for eliciting preferences in a diverse group • Communicate important information regarding the “look and feel” of results
Interactive mapping tool • Users can examine: • How would different kinds of results look? • Can I find a cut point that I like? • Menu allows users to select scenarios • E.g., what would results look like if we had…? • An area in Fresno County • Composed of 100 contiguous census tracts • With twice the expected number of invasive breast cancer cases • With women in other tracts facing the usual risk for invasive breast cancer
Considerations for development of analytic protocol (1) • AG process selected statistical method • Full protocol would include this method plus data management steps before and after to assure validity • Protocol should be something agencies such as CCR could adopt, so consider CCR policies for: • Minimum numbers for cell suppression • Population denominators for between-census years • Procedures for answering public inquiries about rates for non-county areas
Considerations for development of analytic protocol (2) • Complication: Ascertainment of CCR policies difficult • Many are written, but knowledge, interpretation, and adherence to them varies by staff • Many contacts reticent to commit to specific protocols; desire to maintain fluidity depending on source of inquiry and circumstances • Conflicting views about appropriate roles for Advisory Groups in policy development
Considerations for development of analytic protocol (3) • AG: Even if difficult to elicit CCR needs, making protocol and results public may still be helpful • Strategy: Do our best to maintain • Scientific rigor • Replicability • Confidentiality • Usefulness • Adherence to values known to be held by CCR staff
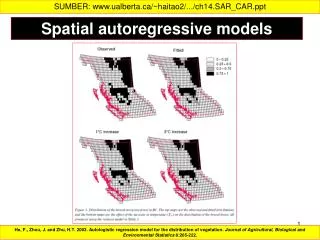
Analytic Protocol • Invasive breast cancer (excludes in situ) among women (age adjusted) by year diagnosed, 2000-2008 • Geography: Census tracts from 2000 • Included steps for denominator calculation, SatScanTM settings • Processing of “raw” results from Scan Statistic—exclude results most likely to arise from • Sudden population shifts • Temporary changes in detection rates
North SF Bay South SF Bay West LA / East Ventura South Orange County boundaries Data Source: California Cancer Registry, 2000-2008 Prepared by the California Breast Cancer Mapping Project Final Areas of Concern North SF Bay South SF Bay West LA / East Ventura South Orange County boundaries
Final Areas of Concern North SF Bay South SF Bay West LA / East Ventura South Orange County boundaries
Analysis of demographic and clinical data • For all four areas of concern: • White women are over-represented among cases compared to the state population • Hispanic women are under-represented • African-American women are diagnosed at a rate proportional to their representation at the state level • Asian women are generally under-represented (but note risk for Asian women varies by sub-group)
Analysis of demographic and clinical data • For all areas of concern exceptWest LA / East Ventura: • Women were slightly more likely to be diagnosed at an earlier stage (i.e. before their cancer had spread) compared to women diagnosed statewide • Women were more likely to have private insurance at the time of diagnosis than women in the state overall
Comparing areas of concern with counties Invasive breast cancer rates aggregated over 2000-2008
Conclusions • Mapping cancer data in this fashion provides information complementary to counties-only approach • No sacrifices for statistical validity, scientific rigor, patient confidentiality
Implications • Design of communication products for results • Publicly accessible report under development • Manuscript under review • General on-line toolkit for accessing and understanding registry data? • Could a protocol similar to this: • Be adopted by cancer registries for routine dissemination of surveillance data? • Be incorporated into CEHTP activities?