Download
1 / 27
290 likes | 767 Views
Thyroid gland diseases 2. M . Alhashash MD. Toxic goiter. Thyroid enlargement with increased thyroid function. Toxic goiter Etiology and Types. Primary thyrotoxicosis (Grave’s dz ) Diffuse vascular goiter appearing hand by hand with toxic manifestation

E N D
Thyroid gland diseases 2. M . Alhashash MD
Toxic goiter • Thyroid enlargement with increased thyroid function.
Toxic goiterEtiology and Types • Primary thyrotoxicosis (Grave’s dz) • Diffuse vascular goiter appearing hand by hand with toxic manifestation • Young age, more in females & with eye signs. • The only autoimmune dz with hyperfunction (females , familial, remission and relapse). • The responsible Ab is TSAb. • Secondary thyrotoxicosis (Plummer’s dz) Hyperfunction occurs on top of simple nodular goiter i.e goiter then hyperfunction. 2 types. • First types : internodular tissue is active (autonomus) and the nodules are inactive. • Second type : one nodule is active (autonomus) and the rest of the gland is inactive called toxic nodule.
Toxic goiter Etiology and Types 3. Toxic adenoma the rest of the gland is not nodular(normal gland). autonomous hyperactive adenoma. 4. Rare types as: • thyrotoxicosisfactitia from excess L-troxine. • Neonatal from the toxic mother. • Struma overii • Pituitary adenoma. • Ectopic thyroid
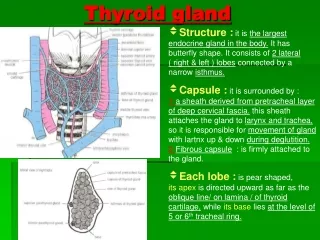
Toxic goiter Clinical picture • The gland • Primary diffuse enlargement , uniform ,smooth ,rubbery , thrill. ( in this type toxic manifestation may present without goiter) • Secondary diffuse or localized ,nodular surface , firm consistency.
Clinical pictureIncreased metabolism • CNS: Sympathetic overactivity • Insomnia. • Nervousness • Anxiety • Tremors • Exaggerated reflexes.
Toxic goiter Clinical picture • General • Progressive weight loss inspite of good appetite. • Hotness intolerance. • Glucose intolerance. • Easy fatigue.
Toxic goiter Clinical picture • Cardiovascular : • Tachycardia • Palpitation • Arrhythmia • Cardiomyopathy • Skeletal weakness • GIT: diarrhea. • Genital : impotence , menorrhagia.
Toxic goiter Clinical picture • Warm , wet skin. • Eye :exophthalmos • Stairing look = infrequent blinking. • Lid lag • Lid retraction • Redness, pain , • Dermopathy : • Non pitting pretibial edema (myxedema only in Grave’s dz)
Toxic goiter Clinical picture • Cardinal signs : • Tremors • tachycardia • Thyroid bruit • Exophthalmos • Moist skin
HYPERTHYROIDISM GRAVE’S Disease (Diffuse Thyroid Goiter) • Triad: • diffuse goiter • thyrotoxicosis • exopthalmos • Other: • hair loss • pretibialmyxedema
Toxic goiter Investigations • Lab : • T3 , T4 , TSH. • TS Ab. • Radiological : • Plain X-ray • U/S • Radioactive iodine uptake RAIU • CT or MRI. • Biopsy. • Laryngoscopy and sleeping pulse.
Hyperthyroidism—uptake • A. Normal • B. Graves’ Dz • C. Toxic Multinodular Goiter • D. Toxic Adenoma • E. Thyroiditis http://embryology.med.unsw.edu.au/Notes/endocrine8.htm
Toxic goiter Diagnosis: • Autonomous thyroid function • Low TSH • Elevated T3 / T4 • Thyroid scan ---> diffuse elevated iodine uptake
Toxic goiter Treatment • Choices: • Antithyroid drugs • Radioactive iodine therapy • Surgery • Choice depends on: • Age • Severity of the disease • Size of the gland • Coexistent pathology (Ophthalmoplegia) • Other factors: • Patient’s preference • Pregnancy
Toxic goiter Medical treatment. • Antithyroid Drugs: • Propylthiouracil (PTU) = 100-300mg TID • Methimazole (Tapazole) = 10-20 TID • Carbimazole = 40mg • Lugol’s iodine. 10 drops TDS • Beta blockers : Inderal. • Tranquillizers.
Toxic goiter Indications of medical treatment. • Small • Mild toxicity • Young age • Primary type • Preparation to surgery • Contraindication to surgery • Recurrence after surgery • Marked eye manifestations.
Toxic goiter Disadvantage of these drugs. • Crosses the placenta --> inhibits fetal thyroid function • Excreted in breast milk • Side effects: • Skin rashes • Fever • Peripheral neuritis • Polyartheritis • Granulocytopenia (reversible) • Agranulocytosis / aplastic anemia (poor prognosis) • Goitrogenic
Toxic goiter Radioactive Iodine Therapy: Advantages: • Avoidance of surgery (no injury to nerve / parathyroid gland) • Reduce cost & ease of treatment Disadvantages: • Lifelong thyroxin replacement therapy • Slower correction of hyperthyroidism • Higher relapse rate • Adverse effect of ophthalmopathy Suitable treatment: • Small or moderate size goiter • Relapse after medical and surgical therapy • Antithyroid drug and surgery are contraindicated Contraindicated: • Pregnant / breast feeding • Ophthalmopathy (progression of eye signs) • Isolated nodular goiter or toxic nodular goiter • Young age (children/adolescence ----> Infertility / carcinoma
Toxic goiter Thyroid Surgery: Indicated to: • Young patient • With Grave’s ophthalmopathy • Pregnant • With suspicious thyroid nodule in Grave’s gland • Large nodular toxic goiter with low level of radioactive iodine uptake. Placed patient to euthyroid state prior to thyroid surgery: • Antithyroid drugs • Lugol’s iodine solution (3 drops BID) • Propranolol
Toxic goiter Thyroid Surgery: Thyroidectomy: • Bilateral subtotal thyroidectomy . • Total lobectomy & subtotal lobectomy contra-lateral. • Total thyroidectomy. Advantages over RAI: • Immediate cure of the disease • Low incidence of hypothyroidism • Potential removal of coexisting thyroid carcinoma Disadvantages: • Complication ---> nerve injury (1%) and hypoparathyroidism (13% transient/ 1% permanent). • Hematoma • Hypertrophic scar formation
Treatment of HYPERTHYROIDISM • Grave’s disease: medical treatment if failed surgery. • Recurrent thyrotoxicosis after surgery---> RAI • Exopthalmos: • Tape eyelids at night • Wear eyeglasses • Steroid eye drop / systemic steroid (60mg prednisone OD) alleviate chemosis. • Lateral tarsorrhaphy to oppose eyelids • Radio-orbital radiation or orbital decompression
Treatment of HYPERTHYROIDISM Toxic Nodular Goiter (Plummers’ disease): • No extrathyroidal manifestation • Milder than Grave’s disease • Treatment: • Propranolol as preparation. • Thyroidectomy (lobectomy with isthmectomy) Toxic nodule: • Surgery. Toxic adenoma • Radioactive iodine
Thyroiditisclassification • Autoimmune • Focal • Diffuse • With goiter = Hashimoto’s dz. • Without goiter =primary myxedema. • Granulomatous = De Quervain’sthyroiditis. • Fibrosing = Riedel’ thyroiditis. • Infective • Acute ( bacterial or viral ). • Chronic (tuberculosis or syphilis).
Thyroiditisclinical picture: • Fever • Malaise. • Thyroid function • Early may be hyperthyroidism. • Late hypothyroidism. • Goiter. Hard gland. • Pressure symptoms. • + or – LN • Suspect malignancy.
Thyroiditistreatment: • L –troxine for replacement. • Corticosteroids for inflammation. • Surgery. • Mass. • Pressure manifestation. • Suspicion of malignancy.
Next :Neoplasms Thanks