Download
1 / 48
510 likes | 612 Views
LEPROSY. HANSEN’S DISEASE DISCOVERED THE ORGANISM IN 1874 CHRONIC INFECTIOUS DISEASE AFFECTING THE COOLER PARTS OF THE BODY. LEPROSY. EXAMPLE SKIN ,MOUTH,RESPIRATORY TRACT,EYES, PERIPHERAL NERVES,SUPERFICIAL LYMPH NODES & TESTIS. LEPROSY.

E N D
LEPROSY HANSEN’S DISEASE DISCOVERED THE ORGANISM IN 1874 CHRONIC INFECTIOUS DISEASE AFFECTING THE COOLER PARTS OF THE BODY
LEPROSY EXAMPLE SKIN ,MOUTH,RESPIRATORY TRACT,EYES, PERIPHERAL NERVES,SUPERFICIAL LYMPH NODES & TESTIS.
LEPROSY BACTERAEMIA FROM ENDOTHELIAL COLONISATION OR BY BACILLI FILTERED FROM BLOOD BY RE SYSTEM, OTHER ORGANS SUCH AS LIVER,SPLEEN ,BONE MARROW & REGIONAL LYMPH NODES ARE ALSO INVOLVED
LEPROSY CAUSATIVE ORGANISM MYCOBACTERIUM LEPRAE LESS ACID-FAST THAN M.TUBERCULOSIS 1. ZIEHL-NEELSEN STAINING –DECOLOURISED BY 5% SULPHURIC ACID 2. FITE – FARACO STAINING 3.GOMORI METHENAMINE SILVER
SLIT SKIN SMEAR TECHNIQUE GIVES QUANTITATIVE MEASURE OF M.LEPRAE STAINED WITH ZIEHL NEELSEN METHOD EXAMINED UNDER 100 x - OIL IMMERSION OBJECTIVE TO DETERMINE THE DENSITY OF ORGANISM IN THE LESION
SLIT SMEAR TECHNIQUE BACTERIAL INDEX –SCORED FROM 1+ TO 6 RANGE FROM 1 TO 10 BACILLI PER 100 FIELDS TO MORE THAN 1000 PER FIELD AS MULTIBACILLARY LEPROSY BI – 0 IS TERMED - PAUSI -BACILLARY
INCIDENCE OF LEPROSY ENDEMIC IN AREAS WITH HOT & MOIST CLIMATES & IN POOR TROPICAL COUNTRIES FIVE COUNTRIES- INDIA,BRAZIL,INDONESIA,MYANMAR & NIGERIA VAST MAJORITY OF CASES INDIA –ONE THIRD OF ALL REGISTERED CASES
INCIDENCE OF LEPROSY IN INDIA – TAMILNADU,BIHAR,PONDICHERRY,AND ANDHRA PRADESH,ORISSA ,WEST BENGAL & ASSAM
MODE OF TRANSMISSION SLOW COMMUNICABLE DISEASE THE INCUBATION PERIOD BETWEEN FIRST EXPOSURE & APPEARANCE OF SIGNS & SYMPTOMS OF DISEASE VARIES FROM 2 – 20 YEARS
MODE OF TRANSMISSION 1.DIRECT CONTACT 2. MATERNOFETAL TRANSMISSION 3.MOTHER’S MILK
CLASSIFICATION OF LEPROSY(RIDLEY JOPLING’S) SEVEN GROUPS TT –TUBERCULOID POLAR(HIGH RESISTANCE) BT- BORDERLINE TUBERCULOID TI – TUBERCULOID INDEFINITE BB –MID BORDERLINE LI- LEPROMATOUS INDEFINITE
CLASSIFICATION OF LEPROSY(RIDLEY JOPLING’S) BL - BORDERLINE LEPROMATOUS LL- LEPROMATOUS POLAR
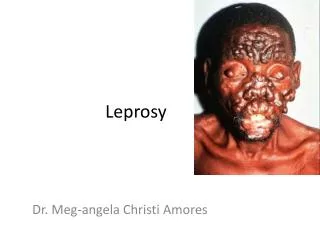
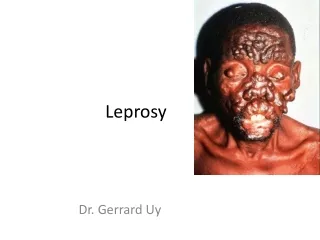
CLINICAL FEATURES OF LEPROSY 2 MAIN FORMS SHOW DISTINCTIVE FEATURES 1.LEPROMATOUS LEPROSY – SKIN LESIONS ARE SYMMETRIC ,MULTIPLE ,SLIGHTLY HYPOPIGMENTED,ERYTHEMATOUS MACULES,PAPULES,NODULES
CLINICAL FEATURES OF LEPROSY NODULAR LESIONS MAY COALESCE TO GIVE A LEONINE FACIES APPEARANCE LESIONS ARE HYPOAESTHETIC OR ANAESTHETIC BUT SENSORY DISTERBANCE IS NOT DISTINCT AS IN TUBERCULOID LEPROSY
CLINICAL FEATURES OF LEPROSY TUBERCULOID LEPROSY SINGLE OR FEW ASYMMETRIC LESIONS & ARE HYPOPIGMENTED & ERYTHEMATOUS MACULES THERE IS DISTINCT SENSORY IMPAIRMENT
HISTOPATHOLOGY OF LEPROSY GUIDELINES 1. CELL TYPE GRANULOMA 2. NERVE INVOLVEMENT 3. BACTERIAL LOAD
HISTOPATHOLOGY OF LEPROSYLEPROMATOUS LEPROSY LEPROMATOUS LEPROSY DERMIS – PROLIFERATION OF MACROPHAGES WITH FOAMY CYTOPLASM,SEEN AROUND THE BLOOD VESSELS,NERVES &DERMAL APPENDAGES
HISTOPATHOLOGY OF LEPROSYLEPROMATOUS LEPROSY AFB STAIN – BACILLI IN GLOBULAR MASSES OR IN PARALLEL FASHION LIKE CIGARETTES IN PACK IN THE FOAMY MACROPHAGES (LEPRA CELLS OR VIRCHOW CELLS)
HISTOPATHOLOGY OF LEPROSYLEPROMATOUS LEPROSY CLEAR ZONE BETWEEN THE EPIDERMIS & THE INFILTRATE IN THE DERMIS EPIDERMIS OVERLYING THE LESIONS IS THINNED OUT ,MAY EVEN ULCERATE
HISTOPATHOLOGY OF LEPROSYTUBERCULOID LEPROSY POLAR TUBERCULOID FORM TUBERCLES COMPOSED OF EPITHELOID CELLS,LANGHANS TYPE OF GIANT CELLS &PERIPHERAL MANTLE OF LYMPHOCYTES
HISTOPATHOLOGY OF LEPROSYTUBERCULOID LEPROSY INFILTRATE HAS PREDILECTION FOR DERMAL NERVES WITH GRANULOMAS & DESTRUCTION OF NERVES NO CLEAR ZONE
3. BORDERLINE LEPROSY 1.BORDERLINE TUBERCULOID(BT) EPITHELOID CELLS, PLENTY OF LYMPHOCYTES NARROW CLEAR ZONE BACILLI ARE FEW & ARE FOUND IN NERVES
3. BORDERLINE LEPROSY 2. BORDERLINE LEPROMATOUS PREDOMINANCE OF HISTIOCYTES,FEW EPITHELOID CELLS.SOME IRREGULARLY DISPERSED LYMPHOCYTES NUMEROUS LEPRA BACILLI ARE SEEN
3. BORDERLINE LEPROSY 3.MID BORDERLINE(BB) EPITHELOID CELLS NO GIANT CELLS SOME LYMPHOCYTES IN THE PERINEURIUM LEPRA BACILLI IN THE NERVES
4.INDETERMINATE LEPROSY NONSPECIFIC CHRONIC DERMATITIS LIKE BUT FOLLOWING FEATURES HELP IN DIAGNOSIS a. LYMPHOCTIC OR MONONUCLEAR CELL INFILTRATE AROUND SKIN ADNEXAL STRUCTURES LIKE HAIR FOLLICLES
4.INDETERMINATE LEPROSY b.NERVE INVOLVEMENT c. AFB STAIN
REACTIONS IN LEPROSY 2 TYPES 1.TYPE 1 – BORDERLINE REACTIONS 2.TYPE II – ERYTHEMA NODOSUM LEPROSUM
TYPE I REACTION POLAR FORMS OF LEPROSY DO NOT UNDERGO CHANGE IN CLINICAL OR HISTOPATHOLOGICAL PICTURE
TYPE I REACTION OCCURS IN PATIENT’S WITH BORDERLINE LEPROMATOUS LEPROSY(BL) ON TREATMENT. UPGRADE OR SHIFT TOWARDS TUBERCULOID TYPE
TYPE I REACTION THE BORDERLINE GROUPS ARE UNSTABLE & MAY MOVE ACROSS THE SPECTRUM IN EITHER DIRECTIONS WITH UPGRADING & DOWNGRADING OF PATIENT’S IMMUNE STATUS
TYPE I REACTIONUPGRADING REACTION ACCORDINGLY THERE MAY BE 2 TYPES OF BORDERLINE REACTIONS 1. UPGRADING REACTION – CHARACTERISED BY INCREASED CELL MEDIATED IMMUNITY
TYPE I REACTIONUPGRADING REACTION HISTOLOGY - INCREASE OF LYMPHOCYTES OEDEMA REDUCED BACTERIAL INDEX
TYPE I REACTIONDOWNGRADING TYPE 2 .DOWNGRADING REACTION CHARACTERISED BY LOWERING OF CELLULAR IMMUNITY
TYPE I REACTIONDOWNGRADING TYPE SEEN IN BORDERLINE TUBERCULOID TYPE DOWNGRADE OR SHIFT TOWARDS LEPROMATOUS TYPE HISTOLOGY –DISPERSAL OF GRANULOMAS INCREASED NUMBER OF LEPRA CELLS
TYPE II REACTION –ERYTHEMA NODOSUM LEPROSUM OCCURS IN LEPROMATOUS PATIENTS AFTER TREATMENT CHARACTERISED BY TENDER CUTANEOUS NODULES ,FEVER,IRIDOCYCLITIS,SYNOVITIS & LYMPH NODE INVOLVEMENT
TYPE II REACTION –ERYTHEMA NODOSUM LEPROSUM HISTOLOGY - INFILTRATION BY NEUTROPHILS & PROMINENCE OF VASCULITIS SECONDARY AMYLOIDOSIS MAY FOLLOW REPEATED ATTACKS
IMMUNOLOGY OF LEPROSY LEPROMIN TEST –INTRADERMAL INJECTION OF LEPROMIN , AN ANTIGENIC EXTRACT OF M.LEPRAE. NOT A DIAGNOSTIC TEST BUT USED FOR CLASSIFYING LEPROSY ON THE BASIS OF IMMUNE RESPONSE
IMMUNOLOGY OF LEPROSY M.LEPRAE REVEALS DELAYED HYPERSENSITIVITY REACTION (BY T HELPER CELLS) IN PATIENT’S WITH TUBERCULOID LEPROSY
IMMUNOLOGY OF LEPROSY 1.FERNANDEZ REACTION –EARLY POSITIVE REACTION- AS AN INDURATED AREA IN 24- 48 HOURS
IMMUNOLOGY OF LEPROSY 2.MITSUDA REACTION - A DELAYED GRANULOMATOUS LESION AFTER 3 – 4 WEEKS PATIENTS OF LEPROMATOUS LEPROSY ARE NEGATIVE BY THE LEPROMIN TEST
IMMUNOLOGY OF LEPROSY LL LACK T HELPER CELLS BUT LL HAVE HIGH LEVELS OF IMMUNOGLOBULINS LIKE IgG,IgA,IgM & ANTIBODIES TO MYCOBACTERIAL ANTIGENS