Download
1 / 43
500 likes | 953 Views
Spinal cord disorders Brains without brawn. Ziv Williams, MD Department of Neurosurgery Massachusetts General Hospital Harvard Medical School. Pathophysiology of spinal cord injury. Primary injury Immediate Axonal injury with loss of nerve conduction.

E N D
Spinal cord disorders Brains without brawn • Ziv Williams, MD • Department of Neurosurgery • Massachusetts General Hospital • Harvard Medical School
Primary injury • Immediate • Axonal injury with loss of nerve conduction. • Damage to oligodendrocytes and myeline sheath leading to reduced nerve conduction.
Secondary injury • Minutes to days. • Wallarian degeneration. • Edema leading to cord expansion and additional compression. • Activation of apoptotic mechanisms (Caspase pathway) • Scar tissue formation from reactive astrocytes and glial scar.
Late injury • Weeks to months. • Glial scar tissue and lack of growth ‘conduit’ within damaged spinal cord. • Lack of sufficient local neurotrophic growth factors. • Brain derived neurotrophic factor (BDNF). • Glial derived neurtrophic factor (GDNF) • Intrinsic myelin associated inhibitors. • Myelin-associated glycoprotein. • Nogo-66 and amino-Nogo. • Limited intrinsic ability to re-grow damaged axons.
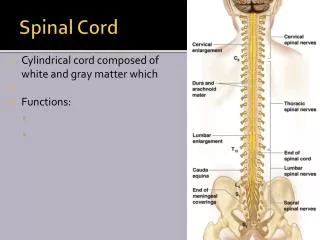
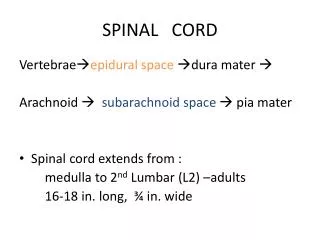
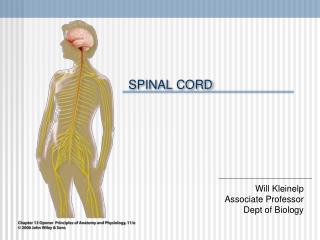
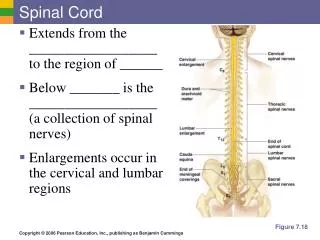
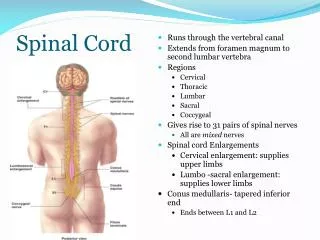
Spinal cord anatomy (brief overview)
Motor control • Corticospinal tract • Responsible for fine voluntary motor control/muscle contraction • From the primary motor cortex, internal capsule, decussates at the level of the medulla, travels to supply the contralateral side
Rubrospinal tract • Responsible for voluntary motor control mostly of large muscles. • Facilitates flexion and inhibits extension of Involuntary limb movement • Red nucleus, decussate in the brainstem, travels to supply the contralateral side • Vestibulospinal tract • Activates proximal limb extensors (anti-gravity) and inhibits flexors for maintained balance and posture. • Vestibular nuclei, anterior funiculus, travels to supply the ipsilateral side
Sensation • Spinothalamic tract • Nociception (pain and temperature) • Decussates 2-3 levels above the dermatome and then travels up ipsilateral cord. Continues as lateral spinothalamic tract.
Dorsal column • Two-point discrimination, vibration and conscious proprioception • Travels up contralateral dorsal column and medial leminiscus. Decussate at the the dorsal column nuclei in the medulla • Spinocerebellar tract • Unconscious proprioception (limb position for posture stability) • Travels up ipsilateral cord, through Clark’s column and terminate in the cerebellum.
Side of injury at the level of the spinal cord • Ipsilateral • Fine and gross motor control • Posture and anti-gravity • Light touch discrimination, vibration and proprioception • Contralateral • Pain and temperature
Strength • Weakness and/or complete paralysis • Loss of descending corticospinal/rubrospinal tracts with preserved muscle bulk and tone • Atrophy and absent muscle tone is rarely seen with spinal cord injury (lower motor neuron or peripheral nerve disease)
Reflex changes • Reflex changes with loss of inhibitory control from descending pathways • Hyper-reflexia – elevated deep-tendon reflex. • Babinski sign –foot and toe extension.
Sensation • Loss of tactile and vibration sensation • Loss of nociceptive sensation • Loss of proprioceptive sensation
Injury overview • Corticospinal pathway damage • Ipsilateral weakness, diminished fine motor control below the level of the lesion. • Hyper-reflexia and Babinski sign. • Dorsal column damage • Ipsilateral loss of tactile discrimination, vibratory, and position sensation below the level of the lesion. • Spinothalamic tract damage • Contralateral loss of pain and temperature 2-3 levels bellow level of injury.
Heritable • Infectious • Inflammatory • Metabolic • Mechanical • Motor neuron
Friedreich’s ataxia • Pathogenesis • Most common progressive spinal ataxia. • Carrier prevalence is 1:100 • Caused by recessive chromosome 9 mutation in the gene coding for Frataxin (necessary for mitochondrial function). • Affects the following • Corticospinal tracts. • Posterior columns. • Spinocerebellar tracts. • Associated with fiber loss and gliosis
Clinical manifestations • Bilateral symptoms • Loss of fine motor control and weakness • Loss of proprioception and discrimination/vibration sensation. • Unsteady gait and teetering/swaying while standing. • Hypo-reflexia • Diagnosis • Clinical manifestation. • Familiar inheritance. • Treatment • Supportive. • Genetic counseling.
Tabes Dorsalis • Pathogenesis • Syphilis (Treponema Pallidum). • Produced by meningovascular inflammation. • Affects the following • Dorsal root of the posterior horn • Posterior columns • Manifests as demyelination and inflammatory changes.
Clinical manifestations • Normally manifest 15-20 years after infection. • Symptoms bilateral and equal. • Shooting and burning pains. • Impaired tactile discrimination, vibratory, and conscious position sensation • Hypo-reflexia • Maintained strength (early). • Diagnosis • Serum treponemal antibodies. • CSF demonstrating elevated lymphocytes. • Treatment • Penicillin infusion. • Symptomatic treatment for pain and gait instability.
Transverse myelitis • Pathogenesis • Often preceded by a viral or upper respiratory illness prior • Acutely evolving inflammatory-demyelinative disruption of the spinal cord. • Affects the following • called ‘transverse’ because it commonly occupies a narrow horizontal band across the spinal cord • Posterior columns • Manifests as demyelination and inflammatory changes.
Clinical manifestations • Characterized by paraparesis or paraplegia that evolves over hours to days. • No clear offending mechanism such as trauma. • Ascending sensory (commonly ascending to the mid trunk level). • Hyper-reflexia. • Diagnosis • Elevated lymphocytes and increase total protein in the CSF (no oligo-clonal bands like multiple sclerosis). • MRI demonstrates a cross-sectional focal edema/swelling of the spinal cord. • Treatment • High dose steroids. • Supportive care.
Subacute combined degeneration • Pathogenesis • Vitamin B12 deficiency. • Essential factor in succinyl CoA metabolism. • Necessary for producing fatty acids in the lipid membranes of myelin • Absorption insufficiency and malnutrition. • Affects the following • Begins in the posterior columns of the lower spinal and peripheral nerves. • Followed by the upper columns and corticospinal tract. • Manifests as patchy loss of myelin and myelin sheath swelling.
Clinical manifestations • Bilateral symptoms • Sensory changes, often come before motor changes. • Loss of vibration, two point discrimination and conscious proprioception. • Lower extremity weakness. • Diagnosis • Serum B12 levels and red blood cell count • Treatment • Vitamin B12 administration. • Treat the source of deficiency. • Recovery depends on the duration of initial symptoms • The greatest improvement occurring in patients with symptoms present for less than 3 months.
Compressive spinal cord injury • Pathogenesis • Mechanical compression • Traumatic bone fragment. • Disk herniation. • Tumor. • Disruption of ascending and/or descending tracts • Clinical presentation • Site and severity dependent
Brown-sequard syndrome • Corticospinal/rubrospinal tract disruption • Ipsilateral paralysis • Ipsilateral hyper-reflexia • Ipsilateral Babinski sign • Dorsal column disruption • Ipsilateral loss of tactile discrimination, vibratory, and proprioception • Spinothalamic tract disruption • Contralateral loss of pain and temperature sensation 2-3 segments below the level of injury.
Complete cord transaction/injury • Initial presentation • Spinal shock normally for the first 1-4 weeks. • Sensory loss in all modalities. • Muscular flaccidity (complete loss of tone and voluntary movement). • Complete loss of reflexes (hypo-reflexia). • Though to occur via transient hyperpolarization and desensitization of spinal cord neurons bellow the level of injury . • Late presentation • Persistent paralysis and sensory loss. • Hyper-reflexia, Babinski sign. • Muscle rigidity.
Diagnosis • Physical exam • Imaging studies (hematoma or bone fragment) • Treatment • High dose steroids for acute compressive injury (limits secondary injury due to edema if given within 8 hours). • Surgical treatment for compressive injury. • Addition of radiation treatment and/or chemotherapy for tumor.
Current treatment options • Medical • Steroids (solumedrol or decadron). • Acute trauma. • Tumor • Transverse myelitis • Vasopressors (neosynephrine or dopamine) . • Acute trauma • Disease specific treatment • Subacute combined degeneration • Tabes dorsalis • Supportive • All cases
Surgical • Bony decompression. • Stabilization (if fracture or bony erosion). • Lesion removal/resection. • Preventative • Trauma prevention. • Genetic counseling.
Stem cell • Autologous pluripotent stem cells. • Induced pluripotent stem cells. • Growth inhibitor antagonists • Nogo receptor antagonists • Promotes myelin regrowth. • Neurotrophic factors • Brain-derived neurotrophic factor (BDNF) • Glial-derived neurotrophic factor (GDNF)