Download
1 / 45
520 likes | 1.23k Views
Basic coagulation techniques and Quality control issues. Dr. Shrimati Shetty Deputy Director National Institute of Immunohematology ( ICMR) KEM Hospital, Mumbai. Final Diagnosis of a bleeding disorder. Anticoagulant.

E N D
Basic coagulation techniques and Quality control issues Dr. Shrimati Shetty Deputy Director National Institute of Immunohematology ( ICMR) KEM Hospital, Mumbai
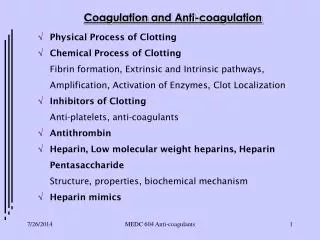
Anticoagulant 0.129 M tri sodium Citrate at a ratio of 9 parts blood to 1 part anticoagulant is used for all coagulation tests. Why not EDTA or Heparin? EDTA irreversibly chelates Ca ions Heparin activates antithrombin which is an inhibitor of coagulation
Anticoagulant… If the HCT is above 55% Anticoagulant vol. [x] = 100 – hematocrit x total vol. of anticoagulated blood required Example: Patient hematocrit = 60% 100 - 60 x 5.0 = 0.37 mL
Preanalytical variables Sample hemolysis/ lipaemic sample Improper proportion of Anticoagulant to blood Prolonged time interval before testing Difficult punctures Freeze thawing the samples
Coagulation Tests • Screening coagulation tests • Confirmatory Tests
When a bleeding patient walks in, what should be the initial tests to be performed? Screening tests Peripheral smear( Bernards Soulier syndrome, macrothrombocytopenia, leukemia , thrombocytopenia ) Complete Blood Count ( BSS, MTCP, Leukemias, thrombocytopenia) PT APTT TT FXIII screening
Only PT is abnormal Congenital Causes Factor VII deficiency Acquired Causes Liver disease Warfarin DIC Inhibitors LA Malignancy
PT - INR • PT measures the deficiency of all VK dependent coagulation factors and also the integrity of extrinsic pathway • INR = [Patient PT]ISI [Control PT]
Only APTT is abnormal Congenital Causes Factor VIII/ IX/XI/XII contact factors Acquired Causes Liver disease Warfarin DIC Heparin Inhibitors to factors, LA
PT & APTT prolonged Congenital causes i.Combined deficiency of V & VIII ii. Factor X deficiency iii. Factor V deficiency iv. Multiple VK dependent clotting factor deficiency Acquired causes Liver disease Warfarin DIC Heparin Inhibitors to factors vitamin K deficiency
PT, APTT, TT prolonged Congenital causes i. Afibrinogenemia/ dysfibrinogenemia ii. Factor II deficiency Acquired causes DIC Liver disease
Screening for F XIII deficiency Clot solubility test Clot formation with either thrombin or CaCl2 Solubility of the clot using 2% acetic acid , 1% mono chloroacetic acid or urea After 24 hours , the clot is observed for solubility Different sensitivities with different clotting reagents & solvents Severe factor deficiency sometimes gets misdiagnosed as F XIII deficiency ELISA test is the sensitive assay for detecting F XIII deficiency
Confirmatory tests-Factor Assays Reagents required Normal pooled plasma or unicalibrator Factor Deficient plasma APTT reagent CaCl2
Factor assays…. Factor VIII/IX/XI/XII – APTT based Factor II/VII – PT mode Factor V/X – can be both PT/APTT mode
Interpretation of factor results At birth, activities of the vitamin K dependent factors II, VII, IX, and X and the concentrations of the contact factors XI and XII are reduced to about 50% of normal adult values. The levels of the factors V, VIII, XIII, and fibrinogen are similar to adult values Plasma concentrations of the naturally occurring anticoagulant proteins (antithrombin, protein C, and protein S) are significantly lower at birth than during the adult years Most blood coagulation factors and fibrinogen increase during pregnancy. Factor (F) XI is the only blood coagulation factor that decreases. Malignancies
Interpretation Should we go ahead with factor assays even when screening tests are normal? yes, in case of any clinical indication we should do the specific factors even if PT/APTT is normal
NPP 20-25 healthy donors , blood group matched Compare it with unicalibrator with known factor values Never use a single individual sample as control
Deficient Plasma& APTT reagents Should have 0% FVIII Negative for TTD/inhibitors Different APTT reagents have different sensitivities
Factor Assays • Severe <1% factor • Moderate 1-5% • Mild 6-40% About 5% of the patients are clinically mild despite having <1% factor
Can we diagnose a patient as HA or HB without doing factor assays? Mixing Studies BaSO4 adsorbed normal plasma, deficient in factors VII, IX, X and prothrombin Aged normal serum, deficient in factors V and VIII, prothrombin, and fibrinogen
Platelet Aggregation tests Highly variable results Diet, Medication, physical activity Platelet receptor studies to confirm diagnosis Always confirm diagnosis by other tests Never give a diagnosis based on platelet aggregation alone!
Disorders diagnosed by platelet aggregation and receptor studies Von Willebrand disease Glanzmanns thrombasthenia Bernard Soulier syndrome Storage pool defect Cyclooxygenase deficiency others
What are the other supporting tests? Platelet receptor studies using antibodies specific for platelet receptors GP 1b/IX for diagnosis of BSS (CD 42) GP IIb/IIIa for diagnosis of GT( CD41, CD61) collagen receptors ( CD36)
Diagnosis of VWD Platelet aggregation with Ristocetin ( 1.25 mg/ml) absent or reduced Type IIb shows increased aggregation with 0.5 mg/ml whereas in normal cases there is no aggregation VWF by Electrophoresis sensitive only for severe def ELISA is the test of conirmation RCof , collagen binding ELISA and Multimer analysis to subtype
Diagnosis of BSS • Giant platelets in peripheral smear • Normal or reduced platelet count • Absence of aggregation with 1.25 mg/ml risticetin • Absence of GP 1b/IX receptors by flow cytometry
Diagnosis of GT • Absence of aggregation with 6uM ADP, 4ug/mL collagen and 0.75mM arachdonic acid • Absence of GP IIb/IIIa receptors by flow cytometry
Storage pool defect • Primary phase aggregation with all agonists
Screening for inhibitors ( Mixing studies) NPP and patient plasma mixed and APTT performed at 0 hour, 1 hour and 2 hour Should exclude Lupus anticoagulants FVIII inhibitors are generally progressive , FIX inhibitors/LA immediate acting
Specialized Investigations • Thromboelastography
Quality control exercises IQC EQC
Case 1 Peripheral smear- giant platelets seen Platelet count 130X103/uL PT – C14 Secs/ P 15 secs ; APTT – C29 secs/P 32 secs; TT – C 16 secs/P 15 secs F XIII - N RIPA – Ristocetin 5% ADP, collagen, AA 90-100% GP1b/IX receptors – highly reduced Diagnosis : BSS Some examples
Case 2 PS – normal Platelets 260X 103/ul PT C14 secs/ P 32 secs APTT C 30 secs P 58 secs TT C 15 secs/ P 16 secs F XIII - N FX 96%; F V 15% F VIII 8% Diagnosis: Combined deficiency of F V and VIII Some examples …..