Download
1 / 15
150 likes | 335 Views
GRANULAR CELL TUMOR OF THE LARINX AND OF THE ESOPHAGUS: REPORT OF TWO CASES. National Congress SIAPEC-IAP September 7-9, 2009 Florence, Italy. Giuseppe Palumbieri palumbierigiuseppe@libero.it. Introduction.

E N D
GRANULAR CELL TUMOR OF THE LARINX AND OF THE ESOPHAGUS: REPORT OF TWO CASES National Congress SIAPEC-IAP September7-9, 2009 Florence, Italy Giuseppe Palumbieri palumbierigiuseppe@libero.it
Introduction. Granular cell tumor (GCT) is a uncommon and nearly always benign neoplasm of presumably Schwann cell origin, with predilection for the skin, the soft tissue and the tongue, while laryngeal and esophageal involvement is fairly rare and their diagnosis is mainly based of histopathologic examination of endoscopic biopsies.
Clinico-pathologic cases. Case 1. A 40-year-old white woman presented with a recurrent smooth sessile tumor of the right vocal cord-subglottic area causing hoarseness (the first lesion revealed five years ago).
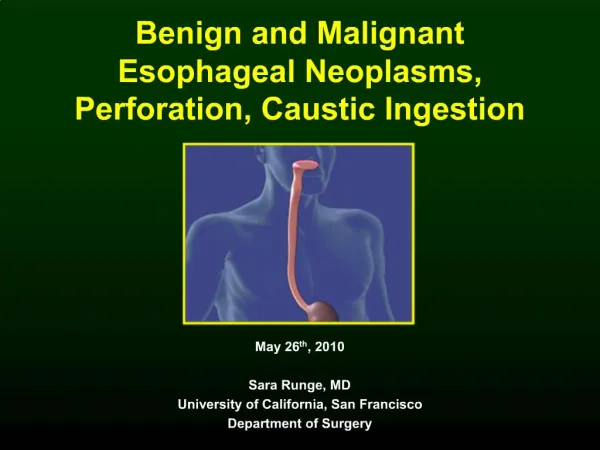
Clinico-pathologic cases. Cause 2. A 42-years-old white man with a flat irregular lesion detected incidentally near the esophago-gastric junction during esophagoscopy: endoscopic diagnosis was Barrett’s Esophagus.
Methods. Tissues were fixed in buffered formalin, paraffin embedded; for immunoisto-chemistry, the avidin-biotin peroxidase complex method was used; antibodies employed are S-100 protein, CD68 (cl. KP1), pankeratin CK-MNF116, CD34 and Vimentina.
Results. Histologically, the tumor was located in the subepithelial area and consisted of sheets of large polygonal and round-oval tumor cells with ample granular eosinophilic cytoplasm and with small round nuclei centrally or eccentrically located, with - in the recurrent tumor of case 1 - nuclear pleomorphism and a few prominent nucleoli: the overlying epithelium was thin and unremarkable in the case 1, while pseudoepitheliomatous hyperplasia is seen in the case 2. The neoplastic cells showed immunoreactivity for S-100 protein and CD68 (KP-1), while ki67-MIB1 was remarkable.
Case 1 Fig. 1 (EE x200)
Case 1 Fig. 2 (EE x630)
Case 1 Fig. 3 (EE x200)
Case 1 Fig. 4 (EE x630)
Case 1 Fig. 5 (S-100 protein x400)
Case 1 Fig. 6 (CK-MNF116 x400)
Fig. 7 (EE x100) Case 2 Fig. 8 (EE x200)
Fig. 9 (S-100 protein x400) Case 2 Fig. 10 (CK-MNF116 x400)
Conclusion. Pseudoepitheliomatus hyperplasia may lead to misdiagnosis as squamous cell carcinoma when a shallow biopsy is performed. Ki67 proliferative index did not distinguish reliably between typical and recurrent atypical GCT. Lastly the endoscopic diagnosis of Barrett’s Esophagus should include GCT.