Download
1 / 1
10 likes | 163 Views
Basal insulin +oral Medication Fasting glucose should be tested once a day before breakfast to titrate insulin plus once a day at different times to identify periods of hypo/hyper Driving-test prior to driving.

E N D
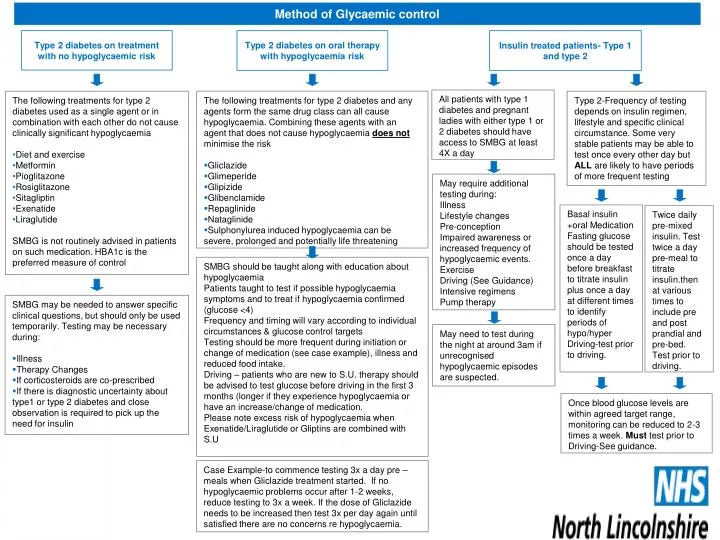
Basal insulin +oral Medication Fasting glucose should be tested once a day before breakfast to titrate insulin plus once a day at different times to identify periods of hypo/hyper Driving-test prior to driving. Twice daily pre-mixed insulin. Test twice a day pre-meal to titrate insulin.then at various times to include pre and post prandial and pre-bed. Test prior to driving. Method of Glycaemic control Type 2 diabetes on treatment with no hypoglycaemic risk Type 2 diabetes on oral therapy with hypoglycaemia risk Insulin treated patients- Type 1 and type 2 All patients with type 1 diabetes and pregnant ladies with either type 1 or 2 diabetes should have access to SMBG at least 4X a day • The following treatments for type 2 diabetes used as a single agent or in combination with each other do not cause clinically significant hypoglycaemia • Diet and exercise • Metformin • Pioglitazone • Rosiglitazone • Sitagliptin • Exenatide • Liraglutide • SMBG is not routinely advised in patients on such medication. HBA1c is the preferred measure of control • The following treatments for type 2 diabetes and any agents form the same drug class can all cause hypoglycaemia. Combining these agents with an agent that does not cause hypoglycaemia does not minimise the risk • Gliclazide • Glimeperide • Glipizide • Glibenclamide • Repaglinide • Nataglinide • Sulphonylurea induced hypoglycaemia can be severe, prolonged and potentially life threatening Type 2-Frequency of testing depends on insulin regimen, lifestyle and specific clinical circumstance. Some very stable patients may be able to test once every other day but ALL are likely to have periods of more frequent testing May require additional testing during: Illness Lifestyle changes Pre-conception Impaired awareness or increased frequency of hypoglycaemic events. Exercise Driving (See Guidance) Intensive regimens Pump therapy SMBG should be taught along with education about hypoglycaemia Patients taught to test if possible hypoglycaemia symptoms and to treat if hypoglycaemia confirmed (glucose <4) Frequency and timing will vary according to individual circumstances & glucose control targets Testing should be more frequent during initiation or change of medication (see case example), illness and reduced food intake. Driving – patients who are new to S.U. therapy should be advised to test glucose before driving in the first 3 months (longer if they experience hypoglycaemia or have an increase/change of medication. Please note excess risk of hypoglycaemia when Exenatide/Liraglutide or Gliptins are combined with S.U • SMBG may be needed to answer specific clinical questions, but should only be used temporarily. Testing may be necessary during: • Illness • Therapy Changes • If corticosteroids are co-prescribed • If there is diagnostic uncertainty about type1 or type 2 diabetes and close observation is required to pick up the need for insulin May need to test during the night at around 3am if unrecognised hypoglycaemic episodes are suspected. Once blood glucose levels are within agreed target range, monitoring can be reduced to 2-3 times a week. Must test prior to Driving-See guidance. Case Example-to commence testing 3x a day pre –meals when Gliclazide treatment started. If no hypoglycaemic problems occur after 1-2 weeks, reduce testing to 3x a week. If the dose of Gliclazide needs to be increased then test 3x per day again until satisfied there are no concerns re hypoglycaemia.