Download
1 / 40
440 likes | 819 Views
Insulin Resistance and Type 2 Diabetes in Children. Brandon Nathan, MD Assistant Professor. Disclosures. I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this CME activity.

E N D
Insulin Resistance and Type 2 Diabetes in Children Brandon Nathan, MD Assistant Professor
Disclosures • I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this CME activity. • I do intend to discuss an unapproved/investigative use of a commercial product/device in my presentation. • Thiazolidenedione and GLP-1 agonist classes of pharmaceuticals in pediatric type 2 diabetes
Objectives Recall the relative differences in prevalence rates for type 1 vs. type 2 diabetes among children of different ethnic backgrounds in the United States Discuss the risk factors that lead to the development of type 2 diabetes in children List the appropriate diagnostic tests to screen an at risk child for type 2 diabetes and the associated metabolic co morbidities of insulin resistance/obesity.
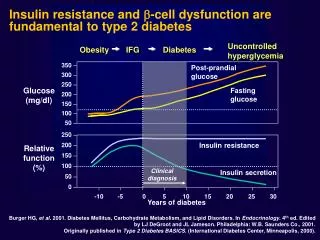
Diabetes Etiology: Insulin Supply,Secretion,Demand Normal Type 1 Pre-type 2 Type 2 Slide courtesy of Toni Moran, MD
Criteria for the Diagnosis of Diabetes or or Prediabetes:HbA1c 5.7-6.4% IFG: impaired fasting glucose (Fasting glucose 100-125) IGT: impaired glucose tolerance (2 hr glucose reading of 140-199 on OGTT)
The Trend in Diabetes is Alarming • 25.8 million people in the US have diabetes (8.3% of population) • Additional 79 million have prediabetes • Overall risk of death twice that of people without diabetes of similar age • Leading cause of blindness, end stage renal disease, non-traumatic leg amputation • 2-4 fold increased risk for cardiovascular disease • Estimated costs in 2007: $174 billion • 1 in 3 children born in the US in 2000 will develop diabetes (CDC) • 50% of African American and Latino children may develop T2DM
Rates of New Cases of Diabetes in US from 2002-2005 Mayer-Davis EJ, et.al. Diabetes Care, 2009
Is Pediatric T2DM a global epidemic? Cohort of 535 obese Italian children IFG (7.6%), IGT (3.2%), T2DM (0.18%) Cambuli, VM, et.al. Diab Metab Res Rev, 2009 Prevalence of T2DM among 0-20 year old German children estimated at 2.3 cases per 100,000. Neu A, et.al. Pediatric Diabetes, 2009 Highest risk populations (obese, Latino, positive fam hx) from Los Angeles from 2000-2007 showed prevalence of 1.3% on OGTT Goran MI, et.al. J Pediatr, 2008 Taiwanese children aged 6-18 taking part in screening program found diabetes prevalence of 9 (♂) and 15.3 (♀) per 100,000 children. After 3 years, 54% of cases identified as type 2. Wei JN, et.al. JAMA, 2003
NHANES suggests an increase in prediabetes and diabetes over past 10 years May AL, et.al. Pediatrics, 2012
Visceral Adiposity Caglecartoons.com
U.S. childhood obesity rates have tripled over the past 40 years Obesity: BMI > 95% Source: CDC (NHANES data)
Obesity rates are highest among adolescents of ethnic backgrounds Prevalence of obesity among boys aged 12-19 years Prevalence of obesity among girls aged 12-19 years Source: CDC (NHANES data)
Popular Teen-Age/Pediatric Grand Rounds Lunch Items… Chipotle Chicken Burrito – rice, black beans, cheese, salsa, grilled chicken 1154 calories Dominos: Slice of Pizza Cheese/Veggie: 290 calories, 9 grams fat Sausage/Pepperoni: 330 calories, 12 grams fat Popular Beverages (Pop, Monster Energy, etc.) 16 oz: 200 calories Starbucks Venti (20 oz) Caramel Macchiato 300 Calories
Risks of obesity increases with sedentary activity Gortmaker S., et.al. Arch Pediatr Adol Med, 1996; 150: 356-62
Diet & Activity Genetic Influences Energy Excess Carbohydrates Fats Carbohydrates b-cell Adipocyte Hepatocyte Oxidative Stress Impaired Insulin Secretion Lipogenesis Steatohepatitis Insulin Resistance Hypertrophy & Hyperplasia Oxidative Stress/ROS Free Fatty Acids Inflammatory Mediators Adipokines • Peripheral Insulin Resistance • Lipid accumulation in peripheral tissues • Endothelial Dysfunction Frohnert B, et.al. Rev Endocr Metab Disord, 2008
Intrauterine environment plays important role in contributing future risk for T2DM Wei JN, et.al. Diabetes Care, 2003
OBESITY • visceral FAMILY HISTORY FEMALE GENDER INSULIN RESISTANCE PUBERTY OTHER GENES Primary Factors Contributing to Development of T2DM in Children T2DM ACCELERATED BETA CELL FAILURE PRENATAL ENVT. IFG/IGT SEDENTARY LIFESTYLE ETHNIC BACKGROUND
Beta-cell secretory abnormalities accompany progression to T2DM Bacha F, et.al. Diabetes Care, 2009
Acute, Life-Threatening Complications of T2DM in Children • Diabetic ketoacidosis (DKA) • May occur in up to 40% of patients • Non-ketotic hyperosmolar coma • 1966-2001: 35 cases reported; 2001-2010: 65 cases • More typical in African-American boys before T2D dx • Characterized by shock, non-acidosis, stupor/coma • Fatality rates ~ 40% (BMI-SDS > 2.9) Rosenbloom A, J Pediatr, 2009 • CHOP: 4.2% of patients over 5.7 year period Fourtner SH, et.al. Pediatr Diab, 2005
T2DM in childhood predisposes for earlier onset of nephropathic disease ESRD IN PIMA INDIANS Pavkov ME, et.al. JAMA, 2006
Co-morbid metabolic conditions are present at high rate in children with T2DM TODAY Cohort (n = 704) Co-morbidityPresent at Baseline Low HDL (♀<50, ♂ <40) 80% High TG (> 200) 10% Hypertension 14% ALT 1.5-2.5 > ULN [>2.5 excluded] 3% Microalbuminuria 13% Copeland KC, et.al. J Clin Endocrinol Metab, 2011
Adolescents with T2DM are at greater risk for rapid deterioration in glycemic control Katz LL, et.al. J Pediatr, 2010
Atherosclerosis begins in Childhood Berenson GS, et.al. N Engl J Med, 1998
Children with T2DM are at increased risk for premature cardiovascular disease • Pediatric Criteria for Metabolic Syndrome (three of five) • Fasting glucose ≥ 110 mg/dl • Waist circumference ≥ 90th % • Triglycerides ≥ 110 mg/dl • HDL-C ≤ 40 mg/dl • 5. Blood pressure ≥ 90% • Other Evidence for Premature Cardiovascular Disease • Increased vascular stiffness • Higher aortic pulse wave pressure • Inflammatory cytokines
Who Should be Screened for T2DM? ADA 2013 • Overweight Children ≥ 10 years or at puberty: • BMI >85th percentile for age and sex • weight for height >85th percentile • weight >120% of ideal for height • Plus any two other risk factors • Signs of insulin resistance: acanthosis nigricans, hypertension, dyslipidemia, PCOS, hx for SGA • Race: American Indian, African American, Latino, Asian American, Pacific Islander • Family history: T2D in 1st or 2nd degree relative • Maternal history: Diabetes or gestational diabetes • Screen every three years:Fasting glucose, HbA1c, OGTT, random glucose + Sx Diabetes Care 2011; 34:S11-S61 Others: Fasting lipid (Dyslipidemia), ALT (NAFLD), total and free testosterone (PCOS), blood pressure
OGTT may help identify youth at greatest risk Monophasic Biphasic Kim JY, et. al. Diabetes Care, 2012
Metformin is only approved oral agent for pediatric T2DM • Reduces hepatic glucose output (inhibits gluconeogenesis) • Facilitates glucose transport in insulin-sensitive tissues • May normalize ovulatory disturbances in girls with PCOS • Safely used in children • Metabolic effects usually apparent within 2 weeks • May improve LDL, TG, ALT and augment weight loss • GI side effects – improved if taken with food and lessen over time • Rare lactic acidosis or hepatic inflammation
Cumulative Incidence of Diabetes in the Diabetes Prevention Program Risk reduction 31% by metformin 58% by lifestyle
Insulin therapy in Pediatric T2DM • Necessary at time of diagnosis if marked hyperglycemia present • Classification of diabetes may not be clear • Adjunct to Metformin and lifestyle interventions • Accumulating evidence that early insulin therapy for T2DM in adults is beneficial • Many preparations and combinations • Basal Insulin such as Glargine (Lantus) or Detemir (Levemir) • Bolus Insulin such as Aspart (Novolog) or lispro (Humalog) for hyperglycemia correction and meal coverage • Premixed Insulin (70/30 or 75/25)
Complementary 2nd line therapies are not approved for Pediatric T2DM Management • 1. AGENTS THAT INCREASE INSULIN SENSITIVITY • Thiazolidinediones: PPARγ activators • rosiglitazone, pioglitazone • α-Glucosidase inhibitors: Inhibit carbohydrate absorption • acarbose, miglitol • 2. AGENTS THAT INCREASE INSULIN SECRETION • Sulfonylureas: Stimulate SUR receptor • glyburide, glipizide, gliclazide, glimepiride • Meglitinides • repaglinide, nateglinide • 3. AGENTS THAT MIMIC INCRETIN PEPTIDES • GLP-1 agonists • Exenitide, liraglutide • DPP-4 inhibitors • Sitagliptin
TODAYs primary objective is to compare the efficacy of three treatment arms on time to treatment failure based on glycemic control in newly diagnosed children with T2DM. The three treatment groups are: • Metformin (500-1000 mg bid) • Metformin (500-1000 mg bid) AND rosiglitazone (4 mg bid) • Metformin plus an intensive lifestyle intervention called the TODAY Lifestyle Program (TLP). • The TLP program is designed to promote healthy, moderate weight loss through changes in diet and increases in physical activity. Intervention phase was completed in February, 2011
Summary The overall prevalence of T2DM in U.S. youth is ~ 1 in 1000 but is increasing, especially in non-Caucasians, surpassing rates of type 1. Rates of diabetes and complications from diabetes in young adults will reach epidemic proportions in near future. While many factors are involved, obesity (visceral) and insulin resistance are central to development of pediatric T2DM. Additional important risk factors include ethnic background, family history, birth history. Screening should include tests for diabetes and for other co-morbidities: FPG, A1c, lipids, fatty liver disease, BP monitoring, PCOS The most important treatment is lifestyle change. May also include metformin, insulin and management of co-morbidities (hypertension, dyslipidemia, etc). Prevention (policy and societal change, medical interventions, identification of new pathways) is paramount to our efforts in combating diabetes now and in the future.
Known and undiagnosed cases of pediatric T2D Undiagnosed cases of pediatric pre-T2D (IGT/metabolic syndrome) “Pre-pre” T2D: insulin resistance with risk factors