Download
1 / 71
770 likes | 838 Views
Pentosan Polysulfate Sodium. 2016. Introduction Pathophysiology Diagnosis Management Strategies Cystopen Summary. Contents. Interstitial cystitis/bladder pain syndrome ( IC/BPS): A prevalent chronic condition that can be challenging not only to diagnose but also to treat

E N D
Introduction Pathophysiology Diagnosis Management Strategies Cystopen Summary Contents
Interstitial cystitis/bladder pain syndrome (IC/BPS): • A prevalent chronic condition that can be challenging not only to diagnose but also to treat • IC/BPS: Enigmatic chronic debilitating syndrome characterized by urinary frequency, urgency & pelvic pain
IC: Introduction • 1st record (1836): A bladder syndrome with symptoms of urgency, frequency & pain was called “tic douloureux” • Dr. Alexander Skene later coined term “interstitial cystitis” while describing chronic inflammatory lesion of the bladder wall • In 1915, Guy Hunner popularized disease by describing symptom complex of chronic bladder inflammation with characteristic bladder wall ulcer, now known as Hunner ulcer. This description was further expanded by Hand, who in 1949 presented varying endoscopic & histopathologic presentations characteristic of condition Chennamsetty A, et al. Curr Infect Dis Rep (2015) 17:454.
Traditionally, interstitial cystitis (IC) has been used to describe syndrome but various terms have been proposed over time, including: Painful bladder syndrome (PBS) Bladder pain syndrome (BPS) IC/BPS & Chronic pelvic pain syndrome (CPPS), further complicating the terminology For consistency purposes, syndrome will be referred as IC/BPS, per the American Urological Association (AUA) guidelines Nomenclature Chennamsetty A, et al. Curr Infect Dis Rep (2015) 17:454.
Bladder disease complex includes a large group of patients with bladder and/or urethral and/or pelvic pain, lower urinary tract symptoms & sterile urine cultures, many with specific identifiable causes. IC/BPS comprises a part of this complex Panel used IC/BPS definition agreed upon by Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction: “An unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder, associated with lower urinary tract symptoms of more than six weeks duration, in the absence of infection or other identifiable causes.” Definition: AUA Guideline Amendment Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Etiologyof IC/PBS: Unknown & is likely variable Pathophysiology has not been fully elucidated Common denominator in IC/PBS: Damage to urothelium, which normally acts as barrier against insults to bladder Various structural & molecular abnormalities can alter urothelial permeability and trigger pathogenesis of IC/ PBS Pathophysiology French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Mucous layer produced by urotheliumprovides shield against noxious solutes present in urine Anionic mucus regulates permeation of cationic solutes into bladder interstitium, especially potassium, which is normally present in urine at levels that are toxic to bladder interstitium Damaged urothelium produces cytokines that activate mast cells in interstitium Pathophysiology French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Diffusion of excess potassium into bladder interstitium through defective urothelium also triggers mast cell activation Activation of mast cells results in cycle of neuronal hyperexcitability leading to secretion of neurotransmitters & triggering further mast cell stimulation and degranulation This process appears to contribute to chronic pain, urgency & frequency experienced by patients Pathophysiology French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Proposed mechanism: IC/PBS MacDiarmid SA, et al. Rev Urol. 2007; 9(1): 9-16.
Normal bladder Normal bladder transitional epithelium with glycosaminoglycan (GAG) layer covering transitional cells Small blue circles represent bound water molecules & wavy lines represent protein backbone Metts JF, et al. Am Fam Physician. 2001 Oct 1;64(7):1199-1207.
Pathophysiology Normal epithelium Dysfunctional epithelium Pain Urgency
Irritating solutes such as K+ GAG layer damage Urothelial damage Irritated nerve Inflammation Snapshot of Pathophysiology
Pathology • Role of histopathology in diagnosis of IC: primarily 1 of excluding other possible diagnoses
Typical Course • IC/BPS is most commonly diagnosed in 4th decade or after, although diagnosis may be delayed depending upon index of suspicion for disease & criteria used to diagnose it • A history of recent culture proven UTI can be identified on presentation in 18% to 36% of women, although subsequent cultures are negative • Initially it is not uncommon for patients to report single symptom such as dysuria, frequency or pain, with subsequent progression to multiple symptoms Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Typical Course • Symptom flares, during which symptoms suddenly intensify for several hours, days or weeks, are not uncommon • A high rate of prior pelvic surgery (especially hysterectomy) & levatorani pain in women with IC/BPS, suggesting that trauma or other local factors may contribute to symptoms • It is important to note, however, that high incidence of other procedures, such as hysterectomy or laparoscopy, may be result of missed diagnosis & does not necessarily indicate that surgical procedure itself is a contributing factor to symptoms Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Co-morbidities • It is also common for IC/BPS to coexist with other unexplained medical conditions, such as: • Fibromyalgia • Irritable bowel syndrome • Chronic fatigue syndrome • Sjogren’s syndrome • Chronic headaches & • Vulvodynia Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Conceptualizing IC/BPS • It is not known whether IC/BPS is a primary bladder disorder or whether bladder symptoms of IC/BPS are secondary phenomena resulting from another cause • Converging data from several sources suggest, however, that IC/BPS can be conceptualized as bladder pain disorder that is often associated with voiding symptomatology & other systemic chronic pain disorders • Specifically, IC/BPS may be bladder disorder that is part of more generalized systemic disorder, at least in a subset of patients Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Conceptualizing IC/BPS • It has been suggested that IC/BPS is member of family of hypersensitivity disorders that affects bladder & other somatic/ visceral organs and has many overlapping symptoms and pathophysiology • Additional hypothesis is that IC/BPS might be just part of continuum of painful vs. non-painful OAB syndrome Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Symptoms • Pain (including sensations of pressure & discomfort) is hallmark symptom of IC/BPS • Typical IC/BPS patients report not only suprapubic pain (or pressure, discomfort) related to bladder filling, but pain throughout pelvis, including in urethra, vulva, vagina and rectum, and in extra genital locations such as the lower abdomen & back • Finally, pain that worsened with specific foods or drinks and/or worsened with bladder filling and/or improved with urination contributed to a sensitive case definition of IC/BPS Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Symptoms • Prototypical IC/BPS patient also may present with marked urinary urgency & frequency but because these symptoms may indicate other disorders, they do not exclusively indicate presence of IC/BPS • Voiding frequency is almost universal (92% of one population) but does not distinguish IC/ BPS patient from other lower urinary tract disorders • Urinary urgency is also extremely common (84% of same population) but urgency is considered to be characteristic symptom of OAB & thus it can actually confound diagnosis Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Symptoms • IC/BPS patients may experience more constant urge to void as opposed to classic ICS definition of a “compelling need to urinate which is difficult to postpone.” • Typically IC/BPS patients void to avoid or to relieve pain, whereas OAB patients void to avoid incontinence • Symptoms of urinary urgency & frequency may precede symptoms of pain • Median time to development of full symptom complex of frequency, urgency & pain was reported to be 2 yrsin 1 study Hanno PM, et al. Journal of Urology. 2015; 193: 1545-1553.
Signs of IC/PBS French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Symptoms of IC/PBS French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Overlap Between OAB and BPS/IC MacDiarmid SA, et al. Rev Urol. 2007; 9(1): 9-16.
Differential Diagnosis of IC/ PBS French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Impact on Quality of Life Pain, urinary urgency & frequency Limitations on sexual intimacy Sleep deprivation Curtailed activities Reduced ability to work Reduced QoL
History of symptoms/ Voiding dairy Symptom screeners: 2 which are O’Leary-SantSymptom and Problem Index10 & Pelvic Pain and Urgency/Frequency Symptom Scale (PUF) Urinalysis / Urine culture: Exclude bacterial infections & other abnormalities Cystoscopy with hydro distension Intravesical Potassium sensitivty test (PST) Anaesthetic bladder challenge (ABC) Urodynamic testing (to r/o other disorders) Biopsy Diagnosis French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
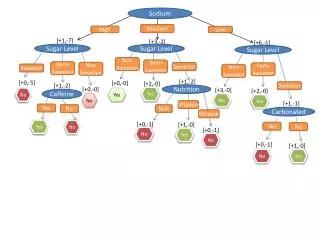
Experience with specific foods & beverages reported by IC/ BPS patients J AcadNutr Diet. 2015_Apr 28.
Experience with specific foods & beverages reported by IC/ BPS patients J AcadNutr Diet. 2015_Apr 28.
Experience with specific foods & beverages reported by IC/ BPS patients J AcadNutr Diet. 2015_Apr 28.
Experience with specific foods & beverages reported by IC/ BPS patients J AcadNutr Diet. 2015_Apr 28.
Medical nutrition therapy algorithm for IC/BPS J AcadNutr Diet. 2015_Apr 28.
A wide array of treatment options exist for IC/ PBS, although well-designed clinical trials to evaluate effectiveness are largely lacking Multimodal therapy that includes pentosanpolysulfatesodium, a tricyclic antidepressant & an antihistamine is a relatively new approach to symptom relief based on advances in understanding of the complementary pathophysiologic mechanisms, but it remains to be evaluated in well-designed clinical effectiveness trials It is important to set realistic goals & expectations with patients because individual responses vary and evidence base is weak Treatment Options French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Pentosanpolysulfate sodium is the only oral therapy approved by the U.S. Food and Drug Administration (FDA) for treatment of interstitial cystitis It was approved in 1996 & is thought to repair urothelium Amitriptyline & hydroxyzine are inexpensive generic medications that also may be used Oral treatment French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Another small RCT demonstrated that oral cimetidine significantly improved symptoms of suprapubic pain & nocturia Limited & uncontrolled studies show pain reduction associated with use of prednisone Other medications: Cyclosporine A, doxycycline, urinary anesthetic (phenazopyridine), alpha blockers, benzodiazepines, muscle relaxants & narcotics Oral cyclosporine has been used to treat IC/PBS based on finding of autoantibodies to urothelium in some patients. Clinically significant improvements were observed, including increased bladder capacity & consequently decreased urinary frequency, but these were in uncontrolled study Oral treatment French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Tanezumab: Humanized monoclonal antibody that specifically inhibits NGF, is important in generation & potentiation of pain following tissue injury and inflammation; NGF signaling inhibition reduces pain-like behavioral pain in several animal models of visceral pain A Randomized, DB study showed that at 6 weeks: Tanezumabproduced significant reduction in average daily pain score & reduction in frequency of urgency episodes along with improvement in global response assessment over placebo Further studies are required to fully understand effects of tanezumab on IC/BPS symptoms Immunotherapy: Tanezumab Chennamsetty A, et al. CurrInfect Dis Rep (2015) 17:454.
A Cochrane review of intravesical therapies identified 9 RCTs using 6 agents 7 including 616 participants (Dawson TE, et al. Cochrane Database Syst Rev. 2007 Oct 17;(4):CD006113.) Therapies identified: Dimethyl sulfoxide Pentosanpolysulfatesodium Oxybutynin BacilleCalmette-Guérin (BCG) Resiniferatoxin & Alkalinizationof urine Intravesical Therapies French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
BCG & oxybutynin seemed most promising and were fairly well tolerated Resiniferatoxinwas associated with increased pain Despite limited clinical trial data, dimethyl sulfoxide is the only FDA-approved intravesical agent to treat painful symptoms of IC/PBS. It is a weakly acidic solvent with anti-inflammatory, analgesic, muscle-relaxant, collagen-degrading& bacteriostatic properties Intravesical Therapies French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Traditionally, irrigation with 50% dimethyl sulfoxide solution is used for 6-8 weeks to relieve moderate to severe painful symptoms of IC/ PBS Women can be taught to self-catheterize & instill premixed solutions at home Intravesical Therapies French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Pentosanpolysulfate sodium can also be used in bladder instillations A small double-blind, placebo-controlled trial including 41 women demonstrated that combination of oral & intravesicalpentosanpolysulfate sodium resulted in significant improvement in moderate to severe IC/ PBS vs. placebo as measured by O’Leary-SantSymptom and Problem Index and health-related quality-of-life measures Alternatively, some experts recommend intravesical heparin Intravesical Therapies French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Intravesical hyaluronic acid is a natural proteoglycan used in Europe & Canada for treatment of IC/ PBS, but it is not approved for this use in US because supporting clinical trial data were lacking An uncontrolled European trial demonstrated that intravesical hyaluronic acid treatments in combination with chondroitin sulfate led to markedly decreased pain and urgency at 12 weeks Intravesical Therapies French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Sacral nerve stimulation Physical therapy may be used in select cases of IC/ PBS, especially for treatment of associated pelvic floor muscle spasm Chondroitin sulfate & quercetin: Postulated to inhibit mast cell degranulation &were associated with symptom reduction when used together in an open-label study. However, RCT data are needed to verify this finding. They are available OTC as dietary supplements alone &in combination Cystectomy with urinary diversion is a treatment of last resort Other Adjunctive Therapies French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
French LM, et al. Am Fam Physician. 2011; 83(10): 1175-1181.
Pentosanpolysulfate sodium, a heparin-like, sulfated polysaccharide, is used to manage bladder pain &discomfort in adults with IC Semi-synthetic which is chemically & structurally similar to heparin and GAG Opaque hard gelatin capsules: 100 mg PPS PentosanPolysulfate Sodium (PPS) Anderson VR, et al. Drugs 2006; 66 (6): 821-835.