Download
1 / 54
540 likes | 670 Views
Cellular Receptors. Chapter 2. Binding of Drugs in/to Cells. Receptor = Drug “target” Membrane protein Enzyme Nucleic acid Most drugs bind receptors by weak, noncovalent forces (what are these?) May be reversed by pH change. Molecular Recognition Specificity. Cellular specificity

E N D
Cellular Receptors Chapter 2
Binding of Drugs in/to Cells • Receptor = Drug “target” • Membrane protein • Enzyme • Nucleic acid • Most drugs bind receptors by weak, noncovalent forces (what are these?) • May be reversed by pH change
Molecular Recognition Specificity • Cellular specificity • Not all receptors in all cells, tissues • Receptors selectively bind partic ligands • Stereoselectivity • No drug completely specific
Ligand/Receptor Interactions • Reversible, bimolecular reaction • D + R DR DR* Response • Where R*=Receptor w/ conform’n change • Each will have rate constant • What does this remind you of??
Activating Drugs = Agonists • Drug/receptor binding • conform’l change in receptor • act’n “downstream” cell biochem pathway(s) • tissue response • May bind at separate site on receptor • “Allosteric modulators” • Increases response to natural agonist
Some definitions • Affinity = tendency to bind receptor • Specificity • Association/dissociation constant • Efficacy = tendency to activate receptor • Full agonists elicit max response • Partial agonists elicit submaximal response
Antagonists Bind Receptors… • BUT no activation occurs • No conform’l change in receptor, so no pathway response • May keep agonists from binding • Competitive • Book ex: curare blocks ACh from receptors of neuromuscular junction inhib’n muscle depolarization paralysis • Allosteric modulators may decrease natural agonist binding • Best antagonists have efficacy=0
Receptor Superfamilies • Ligand-gated ion channels • G protein-coupled receptors • Receptor tyrosine kinases • Nuclear hormone receptors
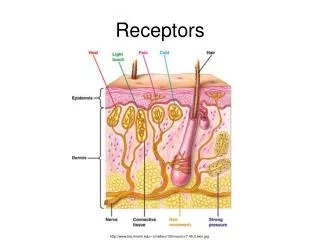
Ligand-Gated Ion Channels • Brain, periph NS, excitable tissues (heart), neuromuscular junction • Nicotinic cholinergic receptors (neuromusc) • GABA receptors (brain) • Glutamate receptors (brain) • change membr potential fast synaptic transmission • Complex prot’s w/ multiple subunits
Book Ex: Nicotinic Receptor • Number of subunits differs w/ tissue • Antagonists differ • Allows selective blockade neuromuscular junction • Multiple binding sites for Ach • Excitatory • incr’d Na+/K+ permeability incr’d depol’n incr’d probability of action potential • Direct transduction (no biochem intermediates)
Allosteric modulators may increase/decrease transmitter response in ligand-gated channels • Ex: benzodiazepines • Antianxiety; sleep disorders • Bind GABA ligand-gated receptors • GABA inhibitory • Increases ability of GABA to open channels
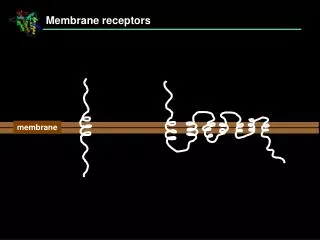
G Protein Coupled Receptors • Single subunit • 7 helices span bilayer • Agonists may bind extracell N-terminal domain, or between helices • Few allosteric modulators known • Cytoplasmic loop couples to G protein
G Proteins • Intermediary mol’s • Bind guanine nucleotides • Extrinsic (periph) prot’s at inside bilayer • Anchored to membr by fa chain • Shuttle between receptor, target prot’s • 3 subunits • GTPase activity by a
“Resting state” G prot – trimer w/ GDP occupying site on a subunit • Agonist binding receptor conform’l change w/in cytoplasmic domain • Receptor acquires high affinity for G prot binding G prot to receptor • GTP replaces GDP • bg duplex dissoc’s from a-GTP • Diffuse along membr • Assoc w/ enzymes, ion channels act’n or deact’n
Term’n activity w/ hydrol Pi from GTP w/ GTPase activity of a subunit • Trimer reunites • Single agonist binding can activate sev G-prot mol’s for sev prod’s/act’n results • Amplification
Sev types G prot’s • Interact w/ diff receptors • Control diff effectors • Gs stim’s enz adenylate cyclase, PLC, others • Gi inhibits ad cyclase, PLC, others • Agonist specificity
Cellular Responses • Amplification of signal through second messengers that activate kinases • cAMP • Phosphatidylinositol • Control regulatory enz’s through covalent mod’n • Large, varied cell responses • GPCRs also control • PLA eicosanoid release • Ion channels depol’n, transmitter release, contractility, etc.
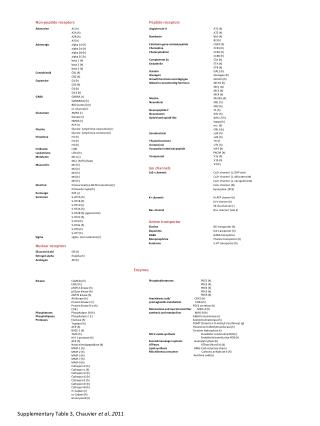
Examples of GPCRs • Receptors for • ACh (muscarinic) • Neuropeptides • Ephinephrine • Muscle (3 types), liver, fat, epithelium, neurons
Receptor Tyrosine Kinases • Single transmembr a helix • Large extracell domain • Agonist binding site • Large intracell domain • Some incorporate tyr kinase activity • Cytokine receptors assoc w/ cytosolic kinases • Agonist binding act’n dimerization • Monomeric form inactive
Dimerized receptors autophosphorylate tyr residues • Phosphorylated tyr attracts, binds SH-2 domain protein • Src Homology • Conserved seq recognizes phosphotyrosine on receptor • Various SH2-domain prot’s allow selectivity for spec receptors • Some are enzymes • Kinases • Phospholipases
Some SH-2 Domain prot’s are couplers for other cell prot’s w/ phosphorylated receptors • Phosphorylation cascades • Impt to cell division, diff’n • Ex: Ras/Raf/MAP kinase pathway • Impt to cancers
SH-2 Domain prot’s as couplers – cont’d • Ex: Jak-Stat Pathway • Impt for cytokines, growth hormone, interferons • Cytosolic kinase phosphorylates receptor dimer • Various Jak’s specificity • SH-2 domain prot’s (Stat’s) attracted, phosph’d, dimerize • Nucleus gene expression
Nuclear Hormone Receptors • Intracellular • Most in nucleus • Some cytoplasmic • Three domains: • Agonist binding domain at C-terminal • Transcriptional control domain • DNA binding domain • Highly conserved • “Zinc fingers”
Ligands lipophilic • Traverse lipid bilayer • Examples: • Steroid hormones • Thyroid hormones • Vitamin D • Retinoic acid • Impt to embryo dev’t
Agonist binding to receptor conform’l change • Dimerization of receptors • Dimers recognize specific base seq’s on DNA near genes • Hormone responsive elements • ~200 bp upstream from genes • Binding DNA may activate or repress gene transcr’n • So “ligand-activated transcr’n factors”
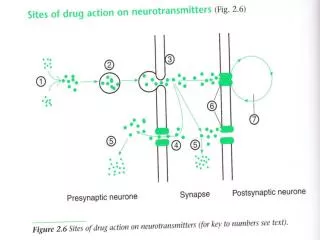
Other Targets of Drugs • Ion Channels • Ligands bind voltage (as well as ligand-gated) channels • Block channel • Affect gating • Activation GPCRs phosph’n channel prot’s • Affect channel opening • Ex: opioids, b-adrenoreceptor agonists • Modulation intracell Ca+2, GTP, ATP • Channels may bind these mol’s • Ex: sulfonylureas act at ATP-gated K+ channels on pancreatic B-cells
Enzymes • Drug may be substrate analog • Competitive or irreversible inhibitor • False substrate • Appears as substrate, so taken up • Not useful as product • Ex: 5-FU blocks DNA synth • Prodrugs • Metabolism active agent
Carrier molecules • Impt for transport across cell membr’s • Have recognition sites for natural mol • Examples: • Cocaine, antidepressants inhibit noradrenaline uptake • Amphetamine acts as false substrate • Loop diuretics affect Na+/K+/Cl- transporter in renal tubule • Cardiac glycosides inhibit Na+/K+ pump
Single Agonist May Have Complex Effects • Families of receptors for agonists • Ex: ACh receptors muscarinic, nicotinic • Further subtypes • Some receptors very specific • Some receptors bind similar ligands • Book ex: dopamine structurally sim to norepi, can stim b1-adrenergic receptors • Multiple receptor subtypes for one ligand can coexist in single cell
Regulation of Receptors • Drugs, agonists decrease sensitivity of receptors to ligands • Fast: desensitization, tachyphylaxis • Gradual: tolerance, refractoriness, drug resistance • Usually w/ continuous exposure • Sensitivity can be increased • Sensitization, desensitization can occur by ligand to same ligand or another
May be due to • Change in receptors • Phosphorylation – inhibits ability to interact w/ G proteins • Slow conform’l change • Exhaustion of mediators • Ex: amphetamines relase amines from nerve terminals; when endogenous amines depleted, drug doesn’t work