Download
1 / 58
590 likes | 941 Views
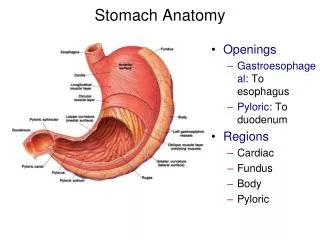
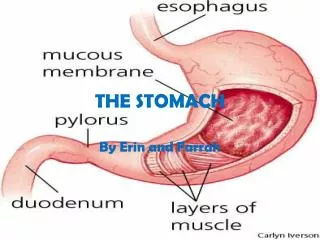
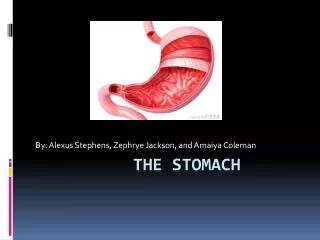
Stomach. Gastric Ulcer Etiology. Acid is less important than duodenal ulcer Lack of mucin and HCO3 secretion Decrease of prostaglandins Decrease mucosal blood flow H pylori infection ( 70%). Gastric Ulcer Diagnosis. UGI endoscpy is mandatory Multiple biopsy and brushings H pylori biopsy.

E N D
Gastric UlcerEtiology • Acid is less important than duodenal ulcer • Lack of mucin and HCO3 secretion • Decrease of prostaglandins • Decrease mucosal blood flow • H pylori infection ( 70%)
Gastric UlcerDiagnosis • UGI endoscpy is mandatory • Multiple biopsy and brushings • H pylori biopsy
Gastric UlcerDiagnosis • Lesion larger than 2.5 cm and located near greater curvature is considered malignant unless proven otherwise • Lesions with everted margins are suspicious for malignancy • Nondistended stomach is suggestive of linitis plastica • Atypia in bx suggest maligancy
Gastric UlcerTypes • Type 1 - 60% of all ulcers, lesser curvature, assoc with blood group A • Type II- 20% , assoc with hypersecretion and duodenal ulcer, blood group O • Type III – 5-10%, prepyloric • Type IV – 10%, within 2cm of GE junction • Type V – assoc with NSAIDs
Gastric UlcerMedical Management • Antisecretory agents • Treatment of H-pylori
Gastric UlcerIndications for Operation • Non healing ulcer • Complication ( bleeding, perforation ) • Morphologic or histologic evidence of malignancy • Failed medical therapy after 3 months
Gastric UlcerPrinciples of Surgical Treatment • In contrast to duodenal ulcer, gastric ulcer should be excised • Vagotomy is indicated only for gastric ulcer asociated with hypersecretion
Gastric UlcerSurgical Treatment • Type I • Antrectomy with Bilroth I is ideal • Excellent results in 90-95% of cases • Type II & III • Antrectomy and vagotomy is ideal • Vagotomy, drainage procedure are alternative therapy
Gastric UlcerSurgical Treatment • Type IV • Excision of ulcer is treatment of choice
Gastric UlcerSurgical Treatment • For complication of gastric ulcer, the ulcer must be excised. • Gastric ulcer must not be patched • Bleeding ulcer should not be oversewn
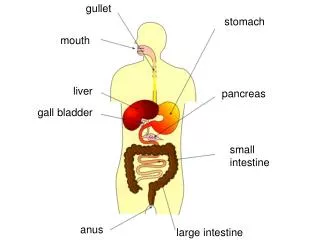
H.Pylori • Gram negative, spiral, motile bacteria • Most commonly involves antrum and lower part of stomach • 20% of population are carriers • 90% infection among duodenal ulcer patients • 70% among gastric ulcer patients
H.PyloriMechanism of Gastric ulcer Formation • Reduces surfactant effect of active phospholipid • This in time reduces gastric mucosal barrier
H.PyloriMechanism of Gastric Cancer Formation • Causes gastritis • Intestinal metaplasia of gastric mucosa • Further progression to cancer
H.PyloriDiagnosis • Breath test ( CLO test ) , non invasive for diagnosis and for evaluation of treatment success • Biopsy – histology and monclonal antibody staining – expensive and invasive • Serology – good for initial diagnosis but not suitable to evaluate for treatment success Urea Hydrolysis H pylori survival strategy in the acid environment of the stomach Urea isbroken down to ammonia and carbondioxide
H.PyloriTreatment • Triple antibiotic with • Amoxicillin • Bismuth sulfate • Flagyl • Tetracycline • Bismuth sulfate • Clarithromycin Simultaneous treatment with anti secretory and antibiotics increases treatment success After adequate treatment a f/u CLO test should be done in 3 weeks
Gastric Neoplasiamalignant tumor • Carcinoma • Lymphoma • Sarcoma • Carcinoid
Gastric carcinoma • More common in males • More common among blacks • Peake age 7th decade
Gastric carcinomaTypes • Intestinal type – associated with mucosal atrophy and intestinal metaplasia • Diffuse type – no known pre-cancerous condition , associated with blood group A and female
Gastric carcinomaEtiology • Pernicious anemia • Adenomatous polyp • Metaplastic change • Diet rich in nitrosurea • H.pylori infection
Gastric carcinomaRole of H.pylori • 90% intestinal , 30% diffuse • Distal gastric cancer
Gastric carcinomaDiagnosis • UGI endoscopy – multiple biopsy and brushing • CT scan of abdomen and pelvis • Endoscopic ultrasound • CEA/CA-125
Gastric carcinomaMorphologic type • Polypoid • Fungating • Ulcerative • Diffuse
Gastric carcinomaHistology • Adenocarcinoma either diffuse of intestinal type • Signet cell carcinoma has poor prognosis
Gastric carcinomaTreatment Two surgical issues • Extent of gastric resection • Extent of lymphadenectomy depends on location of cancer
Gastric carcinomaTreatment of proximal lesion • Total gastrectomy with end to side esophagojejunostomy • Proximal gastrectomy • If tumor extends to lower esophagus – distal esophagectomy with proximal gastrectomy and esophagogastric anastomosis in right chest
Gastric carcinomaTreatment of mid gastric lesion • Subtotal gastrectomy • Routine splenectomy has higher complication without survival benefit • Omentectomy is routinely performed
Gastric carcinomaTreatment of distal gastric lesion • Distal gastrectomy with omentectomy
Gastric carcinomaTreatment for all gastric carcinoma • At least 5 cm margin is desirable • Must do frozen section of prox and distal margins
Gastric carcinomaLymphadenectomy • D1 : resection of the regional perigastric lymph nodes (N1) with the gastric resection. • D2 : resection of the perigastric lymph nodes and those along the feeding vessels (N2) with the gastrectomy specimen
Gastric carcinomaLymphadenectomy • D2 disection does not improve survival over D1 dissection • Higher complication rate with D2 dissection
Gastric carcinomaAdjuvant therapy • No survival advantage of systemic chemo or intraperitoneal chemo • Radiation therapy for high risk gastric cancer reduces local recurrence but does not improve survival
Hiatal Hernia Type I sliding hernia. Type II paraesophageal. Type III mixed hernia The GE junction slides up through the esophageal hiatus during moments of increased pressure in the abdominal cavity. The fixed type implies that there is no sliding up and down. A portion of the stomach remains stuck in the chest cavity. GE junction intact Combination of sliding and paraesophageal
Hiatal Hernia Indication for operative repair of sliding hiatal hernias : symptomatic hernias or complications of GERD
Hiatal Hernia The presence of a paraesophageal hiatal hernia is an indication for surgical repair • bleeding • infarction • perforation
Hiatal Hernia • Based on pathophysiologic studies on patients with a paraesophageal hernia, the repair of the paraesophageal hernia should include an antireflux procedure to correct the sphincter characteristics associated with a mechanically incompetent cardia.
Hiatal Hernia • If time permits, preoperative evaluation with 24-hour pH monitoring and esophageal manometry allows the identification of patients with competent cardias. • Such patients are candidates for simple anatomic repair, provided it can be done without surgical dissection of the cardia.
Rx of Hiatal HerniaAntireflux Repairs: Performed through the abdomen or chest -360 degrees gastric fundus wrap around the lower 1-2 cm of the esophagus
Rx of Hiatal HerniaAntireflux Repairs: 270 degrees gastric wrap generally performed through the chest Belsey-Mark
Rx of Hiatal HerniaAntireflux Repairs: Toupet • 270 degree Wrap
Rx of Hiatal HerniaAntireflux Repairs: Hill posterior gastropexy • 180 degrees wrap performed through the abdomen with the phrenoesophageal ligament anchored to the median arcuate ligament of the diaphragm
Gastric Volvulus Mesenteroaxial • antrum lies above cardia (i.e., rotation around line connecting greater and lesser curvature) • form seen in neonates • usually acute Organoaxial • rare in kids • associated with large hiatus hernia • rotation along long axis of stomach
Diagnosis of Gastrinoma • Fasting hypergastrinemia (>200 pg/ml) in the face of gastric acid hypersecretion defined as basal acid output >15mEq/h • Most patients with gastrinoma have serum gastrin levels >500 pg/ml. • A test is usually done to confirm diagnosis when serum gastrin is in the range of 200-500 pg/ml. secretin provocative Secretin Provocative Test:Following 2 u/kg secretin IV bolus, a rise in serum gastrin level of 200 pg/ml within 15 min or doubling of the fasting gastrin level is diagnostic of gastrinoma.
Diagnosis of Gastrinoma Additional Studies: • Upper GI or endoscopy will show ulcers often in unusual locations, i.e. 2nd & 3rd portions of duodenum or jejunum. The stomach may have prominent rugal folds along with excessive luminal secretions. • CT scan may show tumor in the pancreas or paraduodenal areas. • Angiography with portal venous sampling may show "hot spots" of gastrin secretion
Gastrinoma • 60% of the gastrinomas are non-beta islet cell carcinomas • 25% are solitary adenomas • 10% are microadenomas, or hyperplasia.
Gastrinoma • One-quarter of gastrinomas are associated with the MEN-I syndrome, in which case the tumors are usually multiple and benign. • Sporadic gastrinomas are more often single and malignant. • Even when malignancy is present, the tumors are often slow growing and compatible with a long survival.
Gastrinoma • Over 90% of the patients are adequately controlled with H2-blockers • All patients with sporadic gastrinoma should undergo surgical exploration unless there is evidence of extensive metastatic disease. • The patients with gastrinoma and the MEN-I syndrome have multiple, small pancreatic tumors that cannot be resected, and surgery is generally not indicated. • At operation, the gastrinoma should be enucleated if possible. If not, a distal pancreatectomy may be considered.
Algorithm for the evaluation of a patient with suspected gastrinoma is as follows: • Step 1: Check gastrin level. Measure at least 3 fasting levels • of gastrin on different days. • Step 2: Perform gastric acid secretory studies. A BAO value of greater than 15 mEq/h or a gastric volume of greater than 140 mL and pH of less than 2.0 are highly suggestive of gastrinoma. • Step 3: Perform a provocative test. The secretin stimulation test is the preferred test. • Step 4: Perform somatostatin receptor scintigraphy (SRS). • Step 5: Perform imaging studies to stage and localize the gastrinoma. • Step 6: Determine if patient is a surgical candidate for tumor resection.