Download
1 / 13
130 likes | 348 Views
Funding of Cohort Studies. Diana Finzi, Ph.D. Chief, Pathogenesis and Basic Research Branch Division of AIDS National Institutes of Health Bethesda, Maryland, USA. Cohort Studies. Must reflect current/key research questions

E N D
Funding of Cohort Studies Diana Finzi, Ph.D. Chief, Pathogenesis and Basic Research Branch Division of AIDS National Institutes of Health Bethesda, Maryland, USA
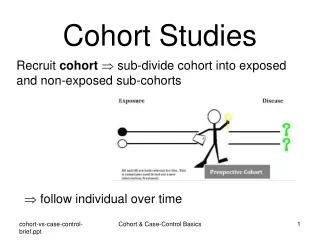
Cohort Studies • Must reflect current/key research questions • Interval-based cohorts were extremely useful in the early days of the epidemic • (Large) clinical cohorts may be more relevant now • Smaller focused studies can be used to address more specific questions • Cost is an issue
Cohort Studies Advantages Disadvantages Expensive Require “ownership”(but problematic if become entitlement) Must strive to stay current Can become unproductive if not managed well • Pool/leverage resources • Can address multiple disease outcomes • Address statistical needs • Accessible to many researchers • Flexible
NIH-funded HIV Cohorts • Multicenter AIDS Cohort Study (MACS) 1984 • Women’s Interagency HIV Study (WIHS) 1994 • Women and Infants Transmission Study (WITS) 1990-2007 • Pediatric HIV/AIDS Cohort Study (PHACS) 2005 • International epidemiologic Databases to Evaluate AIDS (IeDEA) 2005
MACS and WIHS • Anal sex linked to HIV • Low CD4 leads to clinical progression • Effectiveness of anti-retroviral therapies • Identification of long term non-progressors • Detrimental effects of deferring HAART • Link between HHV8 and Kaposi’s Sarcoma • Genetic markers linked to protection (CCR5) • Using hair to measure ARVs
Key Questions • Clinical Research • Long term effects of HIV and ARV with comparisons to HIV-negative controls, taking into account co-morbidities and other exposures (smoking, drug use, alcohol, HPV, HCV, HBV, etc.) • Patterns of therapy use in heavily comorbid patients • Attitudes, beliefs and behaviors • Inflammation and aging • Source of specimens for detailed and exquisitely controlled work • (population level systems biology) • Great breadth of data on 5,000 people • 2.6 m specimens available for WIHS—10% usage • Viral loads, drugs (legal and not), markers, genetics, family history • Diversity of phenotypes at multiple time points
Women and Infants Transmission Study (WITS) • Started in the mid- 1990s, studied natural history of HIV in pregnant women and their children • Stopped in 2007 when transmission rates to infants in the USA reached low levels
Pediatric HIV/AIDS Cohort Study (PHACS) • Effects of perinatally acquired HIV infection in adolescents (sexual maturation, pubertal development and socialization) • Long-term safety of fetal and infant exposure to antiretroviral therapy • With SMARTT look at effects of antiretroviral therapies on uninfected children
NA ACCORD 91,421 Asia/Pacific 6,246 1,416 West 69,705 2,025 East 169,342 29,772 Central 22,190 685 Southern 283,736 30,864 CCASAnet 14,410 900
IeDEA is expanding…. - exposed infected ill therapy death • An evaluation tool for PEPFAR • Development of novel methods for monitoring care • Sentinel sites to measure • lost to follow-up • Pharmacovigilence • HIV negative but ARV/HIV+ exposed children • Measure key indicatorsand feed back into models • Enhanced linkage between care settings • Set data standards for others – to serve as an epidemiologic tool box • TB epidemiology
What now? • Cohorts are a tool to address current HIV questions • When questions are answered such as WITS with matermal/infant transmission, cohorts need to be stopped • When questions change, such as growth of HIV epidemic in Southern US, cohorts need to be changed to address new questions—example of WIHS adding 5 new sites in the South in their 20th year. • US Domestic Cohorts • Need to complete the life trajectory in cohorts • Need to see if next “generation” is the same or different (if same or better we are done) • Support IeDEA • Continue partnerships across ICs, Gates, PEPFAR, MOH, CDC • Develop patient level public health approaches, supported by tools to make evidence based medicine available globally • Support for novel methods –statistics, epidemiology • Support observational research in every corner • Increase epidemiology support to other programs(extend it to TB, hepatitis and other diseases)
Summary • Cohorts come in all shapes and sizes • Must address timely and important research questions • For HIV, the questions have evolved quickly and significantly • What is the scientific question? • Is a cohort the best way to study the problem? • What is the best type of cohort to answer the question? • How will the cohort be maintained? • How can waste and/or excessive spending be avoided? • How will the cohort evolve as questions are answered?
Funding of Cohort Studies Diana Finzi, Ph.D. Chief, Pathogenesis and Basic Research Branch Division of AIDS National Institutes of Health Bethesda, Maryland, USA