Download
1 / 25
350 likes | 1.03k Views
Complications in the Stroke Patient. Mary-Elizabeth Cooper Nurse Practitioner Calgary Stroke Program. Medical Complications. Hypertension Hyperglycemia Elevated Temperature Aspiration pneumonia/UTI GI bleed DVT/PE. HYPERTENSION. Acutely, decrease by NO MORE than 25% from baseline

E N D
Complications in the Stroke Patient Mary-Elizabeth Cooper Nurse Practitioner Calgary Stroke Program
Medical Complications • Hypertension • Hyperglycemia • Elevated Temperature • Aspiration pneumonia/UTI • GI bleed • DVT/PE
HYPERTENSION • Acutely, decrease by NO MORE than 25% from baseline • Be conservative with treatment • Natural decrease in BP within first 24 hours
HYPERTENSION • Chronic treatment aim for BP 135/85 or less on average • Choice of drug less important than target • If choice, thiazide diuretic and ACE-I or ARB should be first choices for stroke patients
HYPERTENSION • Remember to monitor K+ and creatinine to ensure that ACE-I is not precipitating prerenal azotemia • Always consider the cause of hypertension
HYPERGLYCEMIA • Patients who are diabetic or who have elevated blood sugars have a poorer prognosis • Check sugar initially on all patients • Continue monitoring on those who sugars were > 8mmol/ diabetic
HYPERGLYCEMIA • If sugars remain elevated then a sliding scale is appropriate short term • Resume a patient’s regular diabetic meds as soon as is possible • Patients on continuous enteral feeding will not have fasting sugars and goals are different (9-11mmol)
HYPERGLYCEMIA • Like hypertension, stress related hyperglycemia will resolve naturally within 24 hours. • Administer fluids without glucose to stroke patients.
ELEVATED TEMPERATURE • Patients with elevated temperature are more likely to have a poor outcome • Treat all patients with temperature > 38.0 C with acetaminophen • Use cooling measures (fans, cooling blankets) but avoid shivering • Investigate cause of temperature • Can have elevated temperature without infection in intracerebral hemorrhage
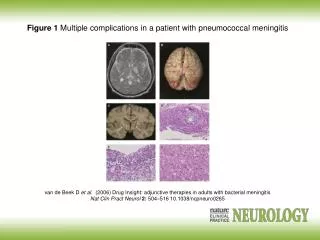
PNEUMONIA • Most common cause is aspiration of oral secretions • Second is inappropriate feeding without proper swallowing screen first • EVERY stroke patient should be assumed to have dysphagia until ruled otherwise
PNEUMONIA • Treatment of choice is Cefazolin 1 gm IV q8h and Metronidazole 500 mg IV q8h • Can switch to oral medication after 48 hours afebrile for a total of 7-10 day course • AVOID cefuroxime (potent inducer of VRE)
URINARY TRACT INFECTIONS • Most are treated with Amoxicillin and Septra (adjust according to culture results) • Avoid unnecessary use of quinolones • Prevent UTI by removing foley catheters as soon as possible • Do not treat asymptomatic bacteruria which is common in older women
GI BLEED • Treat very ill patients and those not eating with Ranitidine 150 mg bid as prophylaxis • Restart PPI’s in patients who have been on them previously ASAP • Initiate feeding either oral or enteral as soon as possible • Avoid NSAIDS in patients on antiplatlet therapy (increase risk bleed, decrease efficacy of ASA)
DVT/PE • Consider all patients confined to bed/chair,or have a hemiparetic leg for DVT/PE prophylaxis • LMWH, enoxaparin 40 mg once daily at 1800 • Intermittent pneumatic compression stockings or TEDS • Among ICH strokes, safe to start LMWH 48-72h after stroke if stable neurologically/systemically • EARLY MOBILIZATION!!!
OTHER COMPLICATIONS • Dysphagia • Malnutrition • Protection of hemiparetic limbs • Falls • Depression • Skin care
DYSPHAGIA • Most common cause of aspiration pneumonia • Present in large proportion of stroke population • Often missed in brainstem or mild strokes • Makes adequate nutritional intake and proper hydration a challenge
DYSPHAGIA • NPO if any doubts and proper swallow screen as soon as possible • May need supplemental feeding and hydration with NG tube • Early involvement of speech and dietician essential • Post signs of diet at bedside for family and staff to ensure safety
MALNUTRITION • Need to start nutrition in whatever form ASAP • Dysphagic patients may require supplemental feeds with NG to meet needs • Requires routine blood work, especially prealbumin to monitor nutritional status • Good nutrition early promotes recovery
PROTECTION OF HEMIPARETIC LIMBS • Needs proper support and positioning at all times • Early intervention by OT/PT essential • Early seating assessment with proper wheelchair • Education of family/patient and staff on proper positioning is key
FALLS/PT SAFETY • Awareness of high risk patients • Proper seating/wheelchair with seatbelt if warranted • Close monitoring of those at risk • Proper mobilization/transfers with appropriate number of staff/equipment • Accurate communication of patient’s risks/needs
DEPRESSION • Continues to go untreated in many stroke patients • Can be confused with flat affect and abulia • Important not to start medication too early • Monitor for warning signs of depression on an ongoing basis • If treatment needed Celexa is drug of choice
DEPRESSION • Reevaluate need for antidepressant over the longer term • Psychology support is important for patient and family during and after recovery • Community support groups are good supports for stroke survivors and their families
SKIN CARE • Proper positioning and turning q2h essential • Early mobilization- get them out of bed!! • Monitor skin frequently for any signs of breakdown, especially diabetic patients • Early intervention with first signs of skin breakdown
FINAL THOUGHTS • EARLY MOBILIZATION!!! • Early involvement of OT/PT/speech • Aggressive management of risk factors • Appropriate referral to stroke rehab