Download
1 / 32
320 likes | 322 Views
This article explores the evidence-based impact of experiential learning in pharmacy education, including the benefits and challenges faced in implementing this approach. It discusses the need for a competency-based curriculum, partnerships with national health systems, and the importance of integrating pharmaceutical and clinical sciences. The article also highlights the role of experiential learning in improving healthcare outcomes, patient experience, and value for money.

E N D
Evidence-based impact of experiential learning Professor Ian Bates Head of Education Development School of Pharmacy University of London
European Directive • 3000 hours of directed study at 4-5 years’ duration • Greater part of curriculum and not less than 50% of final year must be core • At least 35% on actions and uses of drugs • At least 35% on experiments and data analysis • Research project of 3 – 6 months duration
The professional imperative • Better health care, • Better patient experience, • Better value for money
What’s holding us back? • Curricular pressures • Integration of pharmaceutical and clinical sciences • Dislocation of education and practice • Not competency-based • Performance of our graduates? • Not a partnership • With national health systems • With existing health professionals
Short term vs Long term • Long term • The science of medicines must be foundation of education • Knowledge half-life • Short-term imperatives • Understand and engage with the health agenda
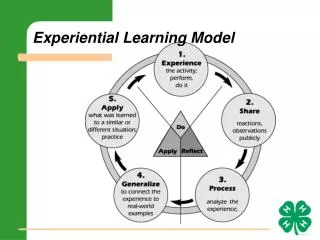
What’s holding us back……curriculum The learning experience Syllabus – knowledge & content Delivery & quality Outcomes Context – institutional, societal & cultural Access, finance & policy
Assessment Goals Independence Good Teaching The Learning Experience… Pharmacy students N = 5,243 p<0.0001 Standardised mean scores
The learning experience • It varies • Is this acceptable? • How can we improve it?
the Knowledge problem …pharmacy syllabus is overcrowded chemistry pharmacology biotechnology genetics medicine analysis formulation physical chemistry ethics pharmacognosy phytochemistry drug design immunology pharmacokinetics therapeutics pathology epidemiology health economics chemical analysis physiology proteomics statistics law Licensing&marketing ADRs microbiology medicinal chemistry biochemistry toxicology drug metabolism genomics social & behavioural sciences
And so…? • Methods • PBL • Near to patient cases • Clinical contact • Experiential • Subject Integration • Designs • Scientists as practitioners • Adult learning & self-direction • Pragmatic & meaningful in situ LLL
“Experiential” learning • Experience • We all have ‘experiences’ • We often learn from an “experience” • Working or work-like • As children…. • Anecdotal…. • No real mysterious or obscure theory
The real issue… …getting the “experience” to UG and PG learners (either students or practitioners) • Design • Environment • Outcomes
…outcomes Competency → Competence → Performance Fit to practise?
performance assessment in vivo performance assessment in vitro clinical context assessment factual assessment Miller’s pyramid From UG to post-registration development Does Shows how Knows how Knows
Experiential learning • Should attempt to bring relevant experience to theory • Should therefore illustrate knowledge (working knowledge?) • Should therefore re-enforce primary learning …it should move learning towards the competency agenda…
Graduation One year later Pharm Care Competencies(OSCE) 70% 60% 60% 50% 40% 30% 30% 20% 10% 1996/97 1997/98 1998/99 2001/02 McRobbie et al
Behaviours Values attitudes Competency Knowledge Skills “Competence” is a complex educational construct… ...with new currency value
An example.. Drug-drug interactions:- • Theory, knowledge • Examples (from lectures, books, case studies, etc) • Exams and questions
Moving from “knowing” (theory)… towards …“doing” (performance)
performance assessment in vivo performance assessment in vitro clinical context assessment factual assessment Miller’s pyramid From UG to post-registration development Does Shows how Knows how Knows
Barriers • Assessment • Resource • Culture
performance assessment in vivo performance assessment in vitro clinical context assessment factual assessment Miller’s pyramid From UG to post-registration development Does Shows how Knows how Knows
Barriers • Assessment • Resource • Culture …there must be a working relationship with the university and the work environment
School Pharmacy Univ Brighton Univ East Anglia Univ Portsmouth Medway School King’s London Univ Reading Kingston Univ NHS Joint Programme Board (JPB)Generalist Training (3 years)www.postgraduatepharmacy.org • Government funding = committment • PG Diploma in General Pharmacy Practice -Core - MI, Technical, Patient & Clinical Services • Common Validation by HEIs in collaborative • Currently 300 practitioner-students (target 2009 = 750)
FDL, e-modes off-site, experiential Independent Career driven Higher Post-reg UG/Pre UG Learning modality with time/career pathway Predominantly FDL and e-modes Predominantly face-to-face modes Cohort learners Lone learner On-site (HEI) learning Off-site (work) learning
General and Higher level practice: Growing the next generation The next [urgent] challenge… • Competency frameworks for undergraduate education • Assessment of performance at UG level (medicines-centered)
The pharmaceutical imperative • Bring our pharmaceutical science into healthcare practice
Where is our professional ‘centre of gravity’? Patient-focussed, medicines-centred ..can only achieve this through a partnership of universities and health care employers (systems)
Key performance indicators F1(medical) Low Activity High Activity W ê ê ê 200 ê W ê ê ê ê 150 W ê W ê ê ê W ê W Pharmacy establishment WTEs 100 ê W ê W W W ê W W W W W ê W ê 50 W W W ê W W W W W W ê W W ê ê ê 0 ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê ê 70 80 90 100 110 120 W W R-Square = 0.16 W W W W R-Square = 0.76 Mortality rate Index
Evidence-based impact of experiential learning Professor Ian Bates Head of Education Development School of Pharmacy University of London