Download

1 / 17
170 likes | 296 Views
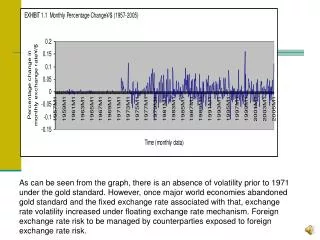
Community Health Centers and Residency Education. Opportunities and Challenges in Partnerships. ADFM Winter Meeting February 19, 2010 Jim Davis Tom Rosenthal Ardis Davis Larry Culpepper Dan Lasser Martha McGrew Patrick Tranmer. What do we hope to accomplish?.

E N D
Community Health Centers and Residency Education Opportunities and Challenges in Partnerships ADFM Winter Meeting February 19, 2010 Jim Davis Tom Rosenthal Ardis Davis Larry Culpepper Dan Lasser Martha McGrew Patrick Tranmer
What do we hope to accomplish? • Focus on “the How”, not “the Why”? • Provide some historical, contextual information on evolving landscape • Illustrate variety of governance models and what works well (or does not work well) about them • Share Lessons learned from partnerships across the county • Leave you with follow-up resources
What is it? • A Combination of existing model of Primary Care Residency and many features of a Health Center (e.g. FQHC) • Designed to create models of community-academic affiliation that promote a shared mission of service and education.
List of Desirables • Medicaid and Medicare reimbursement based on 100% of allowable costs • Cost based reimbursements for educational expenses • EHC is accredited for GME reimbursement • Loan repayment and increased salaries for residents and providers • Funding for EHC startup costs • FTCA coverage extends to all resident and faculty training locations, if desired
Evolution of EHC: The Story • 2004 • The Need: $ viability of WWAMI residency programs • The Situation: Serving as safety net providers but not receiving financial incentives; witnessing “marriages” and “divorces” of FMRs and CHCs; • The Solution: Learn from the affiliations and define a new training entity – an EHC – obtain supporting evidence from quantitative studies of graduates and from qualitative studies of affiliations
Evolution of EHC: The Story • 2005 - 2007 • Quantitative Evidence: Physicians trained in CHCs 3x more likely to work in underserved areas (Morris et al; Fam Med; 2008); yet number and types of these affiliations have not changed in 15 years (Morris et al; Acad Med; in press) • Qualitative Evidence: Common facilitators and barriers are centered around competing missions of service and training, financing, GME policies (Morris et al; Ann Fam Med; 2009) • Documented need for FP workforce in CHCs enhanced advocacy (Rosenblatt et al: JAMA; 2006)
Evolution of EHC: The Story • 2008-2010 • (‘08)Community engagement: Partnership between NWRPCA and UW Dept FM and Residency Network formed (“home” for collaborative work) • (‘09) Increasing legislative advocacy and traction: Teaching Health Center concept (Mullan et al) • (‘09)WAFP Foundation funding $22K (1st grant to partnership to enhance infrastructure) • (‘10) linking partnership to CTSA community engagement activity for expanded grant opportunities
Four Main Barrier Themes • Through EHCI work, 4 themes have emerged and are focus for exploring how to enhance engagement and sustenance of FMR/CHC partnerships. These themes are: • Mission • Money • Quality • Governance/Administration • Panelists will now describe their experience with partnerships along these themes
PANELISTS Dan Lasser – Univ MA Tom Rosenthal - SUNY Buffalo Patrick Tranmer – Univ IL – Chicago Larry Culpepper – Boston Univ Martha McGrew – Univ New Mex
CHC of Buffalo/UBFMA Failed Collaboration 2000-2005 • The 330 Federal Grant was written by the UB Department of Family Medicine. • Mission: Major Source of misunderstanding/ conflict. • UB Family Medicine Goals: • To provide quality primary care to citizens of Buffalo, New York that is of highest quality and is very accessible. • To train family medicine residents in the care of an inner city population of patients in the context of a Federally Qualified Health Center. • CHCB: • Never clearly stated. • Provide jobs for politically connected individuals who are members of the inner city community.
CHC of Buffalo/UBFMA Failed Collaboration 2000-2005 • Money - Not our biggest problem but: • Resources initially improved under the FQHC reimbursements. • CEO increased his salary by 50% • In the first 2 years of operation: • 330 Grant funding received quarterly. • The 330 money was spent within weeks of being received. • New employees hired and then laid off later in the quarter. • Medical School Dean sends in an in house investigator to review billing procedures in CHCB. • Dean failed to perceive nuance of providing physicians under contract. • University had no right of access to records. • Dean reports CHCB to Medicare Fraud investigation.
CHC of Buffalo/UBFMA Failed Collaboration 2000-2005 • Governance • Board Membership: • UB Family Medicine had one designated seat on the board. • A faculty member working at the site assumed this seat but became ill and relatively inactive. (Big Mistake #1) • Community Board members more closely aligned with previous CHC than evident. • Slow to react to seemingly obvious problems.
CHC of Buffalo/UBFMA Failed Collaboration 2000-2005 • First CEO: • Former junior faculty member who was active in writing the grant but not qualified for being the CEO. Appointed to the position by the Board at their first meeting. No search was done. • Later received the clinical diagnosis of Narcissistic Personality Disorder. • Fired after 2 years. He has since lost his license to practice. • Interim: 12 months with interim leadership. • The CHC and Residency thrived. • Money, patient population, residents education, recruitment, faculty satisfaction were all going well.
CHC of Buffalo/UBFMA Failed Collaboration 2000-2005 • Second CEO: Another Narcissistic Personality Disorder, but more organized with higher control needs. • Refused to pay entire half day session if UB FM MD was 10 minutes late. • Purchased an EMR without physician input. • Presented revised contract and refused negotiation. • Canceled CHC maternity care privileges for family physicians. • Hospital and UB Department Chair meet with Board Chairperson - meeting viewed as insubordination by CHC Board and CEO. • 2005: UB Family Medicine Submits 90 day notice of withdrawal from site. • Hospital leases 6,000 square feet in plaza 2 miles from hospital for new FMC. • Hospital revenues from practice increase. • Hospital CEO served eviction notice to CHC. • Second CEO Fired After 2.5 years: Reign of Terror • High employee turnover and patient visits plummet . • Inability to recruit physicians to replace University family physicians.
Resources EHCI Website: http://www.nwrpca.org/education-health-center-initiative.html Others