Download
1 / 9
90 likes | 315 Views
Tonsillitis. By: Maryam Mofarrah Veronica Ratevosian & Sara Golfiez. Chief Complaint . Patients presents with the complaint of ongoing “throat pain”. Patient History.

E N D
Tonsillitis By: Maryam Mofarrah Veronica Ratevosian & Sara Golfiez
Chief Complaint • Patients presents with the complaint of ongoing “throat pain”
Patient History • A 7-year-old girl presented with a 3-year history of recurrent episodes of tonsillitis manifesting with fever, sore throat, fatigue, and poor appetite. She had been treated with a variety of antibiotics. She also had had two episodes of scarlet fever associated with the tonsillitis. Four times during the past year, the results of throat cultures were positive for group A beta-hemolytic streptococcus (GABHS). Additionally, the patient was reported to have noisy mouth breathing, snoring, problems breathing at night, and dysphagia. Her symptoms became significantly worse when she became acutely ill. The patient saw her physician, took antibiotics, and missed 3 days of school.
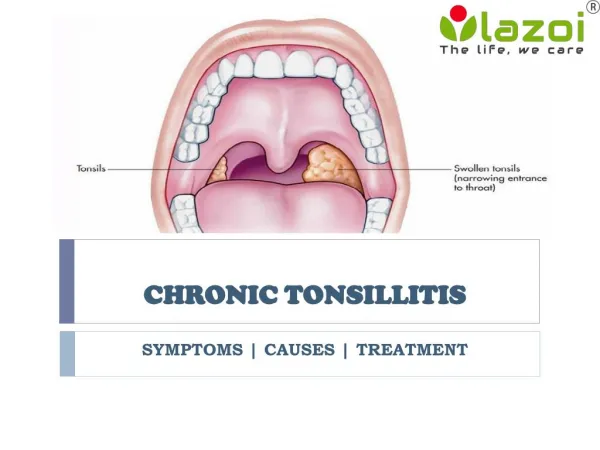
Physical Examination • On presentation, the patient was afebrile and stable with normal vital signs. General appearance revealed a healthy girl with noisy open-mouth breathing, an elongated face, and protruding elongated narrow maxilla with a high-arched palate indicative of adenoid enlargement. Examination of the ears was normal. Examination of the mouth and throat revealed enlarged, cryptic tonsils. Nasal examination indicated slightly inflamed nasal mucosa. Nasal endoscopic exam revealed enlarged adenoids with obstruction of the posterior nasal choana and nasopharynx. On examination of the neck, several shotty lymph nodes were found. The remaining physical examination was normal. A review of the patient’s systems, social history, and past medical history was unrevealing.
Treatment/ Follow-Up • Tonsillectomy and adenoidectomy were recommended after a lengthy discussion regarding the indications, alternatives, risks, complications, and outcome. The patient underwent tonsillectomy and adenoidectomy using Coblation, a soft-tissue surgery system. She was discharged from the hospital the same day of the procedure. • At 3-week follow-up, her breathing and sleeping had improved, she no longer snored, and was able to eat and swallow without difficulty. Her mother indicated that she had to use the prescribed pain medication only once per day for the first 4 postoperative days. The tonsillectomy sites were well healed. There were no abnormal findings.
Discussion • Tonsillectomy and adenoidectomy are among the most common procedures performed under general anesthesia in children every year. More than 400,000 tonsillectomies and adenoidectomies are performed annually in the United States. When these procedures are performed for the proper indications with appropriate technique, updated instruments, and specialized professionals, they have proved to be effective in significantly improving the quality of life of these patients.2 However, many physicians may be uncomfortable or unfamiliar with tonsillitis, current techniques, or results and may make inadequate recommendations, comments, or decisions regarding tonsillectomy and adenoidectomy.
Discussion Continued • The indications for tonsillectomy include a variety of conditions. In the majority of cases, hyperplastic enlarged tonsils and adenoid tissue occupy a disproportionate space of the upper airway in preschool children, resulting in obstruction of the upper airway and manifesting as heavy snoring, difficulty breathing, and sleep disturbance. Symptoms may range from a mild form of airway obstruction known as upper airway resistance syndrome (UARS) to the more severe obstructive sleep apnea syndrome (OSAS). Adenoidectomy/tonsillectomy is considered first-line therapy for these patients. Usually, patients with tonsil and adenoid hyperplasia also present with dysphagia and hyponasal speech or muffled voice. Additionally, abnormal dentofacial growth, e.g., vertical elongation of the face with high, narrow palate vault and a secondary posterior dental cross-bite, may occur.