Download

1 / 34
430 likes | 1.27k Views
Presented To: Our Respected Sir Amir Riaz Sir Khalid Tipu Presented By:. Tonsillitis is an inflammation of the tonsils caused by bacterial or viral infections.

E N D
Presented To:Our Respected Sir Amir Riaz Sir Khalid TipuPresented By: / 42
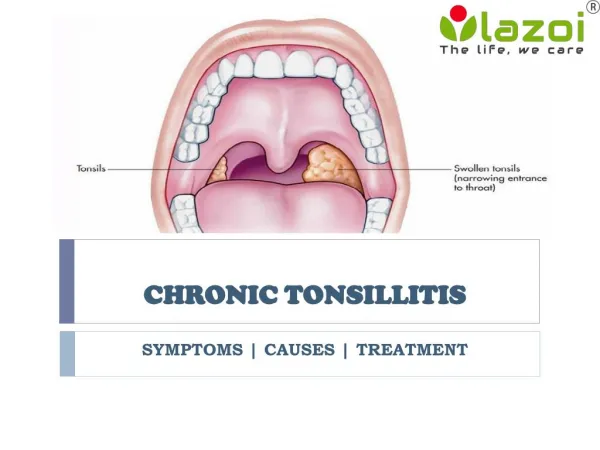
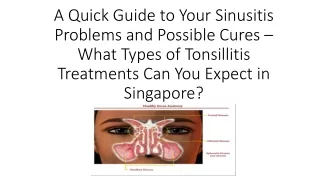
Tonsillitis is an inflammation of the tonsils caused by bacterial or viral infections. Acute tonsillitis is an infection of the tonsils caused by one of several possible types of bacteria or viruses. Chronic tonsillitis is a persistent infection of the tonsils and can cause tiny stone formation. TONSILLITIS / 42
Anatomy of tonsils / 42
Anatomy of tonsils • Tonsils (palatine tonsils) are a pair of soft tissue masses located at the rear of the throat (pharynx). • Each tonsil is composed of tissue similar to lymph nodes, covered by pink mucosa (like on the adjacent mouth lining). • Running through the mucosa of each tonsil are pits or depressions, called crypts. • The tonsils are part of the lymphatic system, which helps to fight infections. / 42
Classification of Tonsillitis • Follicular tonsillitis: tonsillitis especially affecting the crypts. • Parenchymatous tonsillitis that affecting the whole substance of the tonsil. • Pustular tonsillitis a variety characterized by formation of pustules. • Lacunar tonsillitis: inflammation of the mucous membrane lining the tonsillar crypts. / 42
CAUSES • Bacteria • Streptococcus pyogenes • Group C and G beta hemolytic streptococci • Arcanobacterium haemolyticum • Yersinia enterocolitica • Anaerobic infection (Vincent’s angina) • Mycoplasma pneumoniae • Chlamydophila pneumoniae • Neisseria gonorrhoeae • Corynebacterium diphtheria • Viruses • Rhinoviruses • Coronaviruses • Parainfluenza viruses • Adenoviruses • Influenza viruses A and B • Herpes simplex type I (rarely type II) • Coxsackie viruses • Epstein-Barr virus / 42
Causative organisms • < 3 years • 100 % viral • 5-15 years • 15-30 % GABHS • Adult • 10 % GABHS / 42
EPIDEMIOLOGY • Spreads by close contact and through air • Spread more in crowded areas ( school, army..) • Most common among 5-15 age group • More frequent among lower socio-economic classes • Most common during winter and spring • Incubation period 2-4 days / 42
PATHOPHYSIOLOGY • Under normal circumstances, as viruses and bacteria enter the body through the nose and mouth, they are filtered in the tonsils Within the tonsils, white blood cells of the immune system mount an attack that helps destroy the viruses or bacteria, and also causes inflammation at that site. / 42
Sore throat Anterior cervical LAP Fever > 38 C Difficulty in swallowing Headache, fatigue Muscle pain Nausea, vomiting Viral tonsillitis Having additional rhinitis, hoarseness, conjunctivitis and cough Signs/symptoms • Tonsillar hyperemia / exudates • Soft palate petechia • Absence of coughing • Absence of nose drip • Absence of hoarseness / 42
GABHS EBV Adenovirus Primary HIV infection Candida albicans Francisella tularensis Exudates / 42
CLINICAL EXAMINATION • Pharyngeal mucosal diffuse congestion, • The mucosal membrane of the fauces is bright red, • Uvula edema, • The crypt filled with debris, • Desquamated epithelium and pus. • Lymph nodes: below the jaw draining the tonsillar area are frequently enlarged and tender / 42
Throat culture Rapid antigen test If negative need swab WBC count Peripheral smear Laboratory Diagnosis / 42
Throat Culture • Pathogens looked for • Group A beta hemolytic streptococci • C. diphteriae (rare) • N. gonorrhoeae (rare) / 42
COMPLICATIONS ● Local Complications: • peritonsillar abscess (most common seen), retropharyngeal abscess (seldom seen), acute sinusitis, • acute otitis media, • acute laryngitis, etc. / 42
COMPLICATIONS • ● General Complications: • rheumatic fever, • acute glomerulo-nephritis, • acute arthritis, • myocarditis, • Type III allergic reaction, • bacterial toxin / 42
Tonsillitis due to Streptococci • Supurative complications • Abscess & stone formation • Sinusitis, otitis, mastoiditis • Scarlet Fever • Toxic shock syndrome • Cervical lymphadenitis • Septic arthritis, osteomyelitis • Recurrent tonsillitis/pharyngitis • Nonsupurative complications • Acute romatoid fever • Acute glomerulonephritis / 42
Preventive measures • Covering mouth and nose when sneezing or coughing • Washing hands frequently • Washing dishes and utensils used by the infected individual frequently • Keeping dishes, utensils, and other household items used by the infected person separate from those used by other family members • Do not share food or drinks with the infected individual / 42
Aim of Treatment • Prevention of complications • Symptomatic improvement • Bacterial eradication • Prevention of contamination • Reducing unnecessary antibiotic use / 42
Treatment 1) Non-surgical Therapy: Medicine Management, Diet plan Other measures 2) Surgical Therapy: Tonsilectomy. / 42
Diet planBreakfast:Fresh fruites or juices & a glass of milk.Lunch:A bowl of boiled vegetables.Dinner:A bowl of fresh salad. / 42
LOCAL TREATMENT; LozengesOTHER MEASURES: 1. Apply heating compress to the throat. 2. Gargle the throat with hot water, mixed with a little salt And lime juice, several times daily. 3. Massage the throat. 4. Take warm-water bath.5. Fresh air, deep breathing and other exercises. / 42
SURGICAL THERAPY Tonsilectomy: Tonsilectomy is the surgical removal of tonsillitis. / 42
. • This function may make persons particularly vulnerable to infection and inflammation. The problem is more common in children because the immune system function of tonsils is most active before puberty / 42
Major Indications for Tonsillectomy • Indicated as if • (1) persons is with repeated or persistent infections as if there are: • More than five to seven episodes in one year • More than four episodes a year over two years • More than three episodes a year over three years / 42
Major Indications for Tonsillectomy • (2) when serious complications of infection occur; • (3) when enlargement of the tonsils causes breathing, swallowing, or dental problems • (4) A bacterial infection causing tonsillitis doesn't improve with antibiotic treatment / 42
Risks of Tonsillectomy • Swelling of the tongue and soft roof of the mouth (soft palate) can cause breathing problems • Bleeding can occur during the healing process • Rarely, surgery can lead to an infection / 42
Recovery time for tonsillectomy: Recovery time for tonsillectomy is at least one week. Adults may need more time than children. Note:It's important to get plenty of fluids after surgery. Water and ice pops are good choices. Avoid milk for the first 24 hours after surgery. / 42
REFERENCES • Current medical diagnosis &treatment • 2010. • www.druginfo.com • www.answer.com • www.medicinenet.com • Basic and clinical pharmacology by Katzang / 42