Download
1 / 35
350 likes | 546 Views
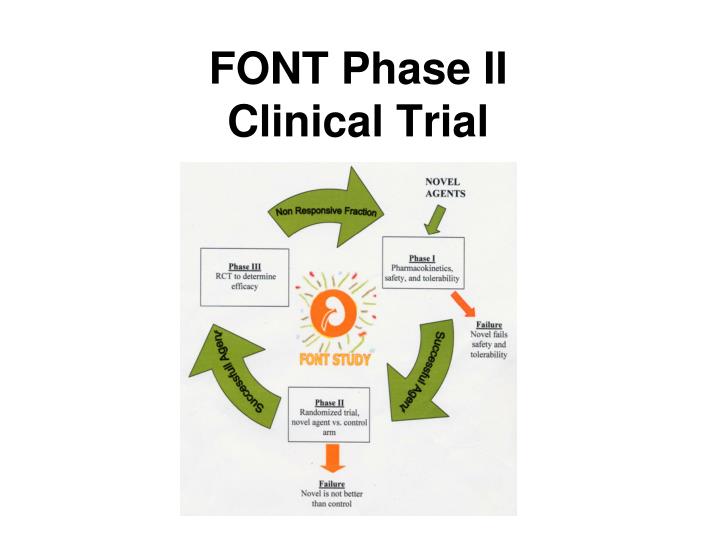
FONT Phase II Clinical Trial. Justification for Novel FSGS Therapy Poor Survival for Resistant FSGS. b. Adult FSGS. a. Pediatric FSGS. CR 12 12 8 5 5

E N D
Justification for Novel FSGS TherapyPoor Survival for Resistant FSGS b. Adult FSGS a. Pediatric FSGS CR 12 12 8 5 5 PR 20 18 13 11 9 NR 28 25 20 10 9 Presler/Gipson, 2005 Troyanov, JASN, 2005
FSGS Clinical Trial: CSA vs. MMF/ Dexamethasone Week Randomize Pred +ACEi 0 26 52 78 CSA MMF + Dex Primary Outcome 6 months ACEi Secondary Outcome Gipson et al, 2011
Eligibility Criteria • Inclusion • Age 2 – 40 years • eGFR ≥ 40 ml/min/1.73m2 • Up/c > 1.0 • Steroid resistance • Biopsy confirmed primary FSGS • Exclusion • Prior therapy CSA, Tacrolimus, MMF • Obesity • Transplant • Malignancy • Diabetes mellitus Gipson et al, 2011
Primary Outcome: Week 52 Proteinuria Remission OR<1 favor CSA Gipson, 2011
FSGS CT: Secondary Outcomes • 6 months after immunosuppression withdrawal • Proteinuria relapse was common (CSA 33%; MMF/DEX18%) • No difference in proteinuria remission status OR= 1.21 (0.56-2.66) Gipson et al, 2011
Adverse Events * * Percent * * * Gipson et al, 2011
www.fonttrial.org Trachtman et al, 2011 Trachtman 2011
Specific Aims 1. To evaluate two novel therapies for resistant FSGS -- anti-TNF-α antibody and galactose against standard therapy 2. To identify one or more novel agents as candidates for future study in a Phase III randomized clinical trial 3. To develop a network of sites to foster the performance of clinical trials for this disease and other glomerular disorders Trachtman et al, 2011
Eligibility criteria • Age 1-50, • GFR >40 mL/min/1.73 m2 • FSGS on bx OR genetic mutation • Steroid resistance • Resistance to a 2nd immunosuppression Trachtman et al, 2011
FONT II REVISED PROJECT Eligible Patients with Resistant FSGS RANDOMIZATION Adalimumab N=17 Standard Rx N=17 Galactose N=17 Pause for Efficacy Review ≥2/17 with Up/c<50% baseline and stable GFRe YES, continue recruitment to N=42* NO, discontinue study arm Trachtman et al, 2011
Standard Conservative Therapy Trachtman et al, 2011
TNF- • Inflammatory cytokine • Produced by circulating or infiltrating mononuclear cells, macrophages, and kidney mesangial cells • Postulated mechanisms • recruitment of leukocytes to the site of glomerular injury • induction of cytokines and growth factors • generation of oxygen radicals resulting in increased glomerular endothelial cell permeability to albumin • direct cytotoxicity to glomerular mesangial and epithelial cells, and induction of apoptosis • Increases in TNF- α and TNF- α mRNA described in FSGS Trachtman et al, 2011
Phase I Adalimumab • N=10 (4M:6F) • Age 16.8±9.0 yr • GFRe 105±50 mL/min/1.73 m2 • Dose 24 mg/m2 (max: 40 mg) sc q 14 d • Up/c 15.9±10.4
Adalimumab: PKThe half life, area under the curve, and clearance were increased in proteinuric FSGS compared with patients with rheumatoid arthritis Joy, 2009
Adalimumab Safety • 9 Adverse Events • 1 probably related: injection site reaction • No discontinuation due to adverse event • Relationship of T1/2 to Up/c and albumin • Treatment Satisfaction Questionnaire for Medicine (effectiveness, side effects, convenience, global satisfaction) • Scores: 61, 92, 71, 59 out of a possible 100
Phase I: Long-term follow-up Trachtman, 2009
Adalimumab: Dosing • Provided by Abbott • Injectable • 40 mg/0.8 mL • Boxes of 6 vials • Dose: 24 mg/m2 SC Q 14 days • Apply EMLA or ice to relieve pain
Circulating permeability factor(s) in FSGS Evidence: Early post-transplant recurrence of proteinuria Proteinuria after injection of FSGS plasma Clinical benefit of plasmapheresis (PP) Permeability activity:In vitro glomerular albumin permeability (Palb) predicts recurrence. Palb of patient specimens 1st & 2nd 1 PP rx IV Galactose Savin VJ, et al., 2008
Permeability is increased most by serum from FSGS patients with severe disease or recurrence after transplantation Palb 1. Savin, NEJM, 1996 2. Butcher, ASN, 1998 3. McCarthy, ASN, 1997 2 3 1 1 1
More rapid progression to kidney failure is seen in patients with high activity (Pudur) 1.0 .75 Low activity, about 40% good function after 5 years Palb < 0.5 Survival distribution Function .50 High activity, only about 25% good function after 5 years .25 Palb 0.5 5 years 0.0 0.0 2.5 5.0 7.5 10.0 12.5 15.0 Time from diagnosis to ESRD, years
Permeability activity is decreased by galactose • Galactose taken twice daily in water. • Activitydecreased at 2 weeks and remained low. Pre-treatment Palb 1 week 4 weeks after stopping galactose 2 weeks 4 weeks 6 weeks Savin VJ, et al., 2008
Galactose and Potential Mechanisms of Action FSPF • Permeability factor may gain access to podocyte by sugar binding. • Galactose may block the binding between factor and podocyte. • Factor-galactose complex may be removed by specific receptors in liver or other tissues. Filtration slits Podocytes galactose galactose galactose FSPF FSPF galactose galactose FSPF FSPF-galactose complex FSPF-galactose complex Galactose receptors Savin VJ, et al., 2008
Cardiotrophin-like cytokine (CLC-1) is present in plasma of a patient with recurrent FSGS Patient plasma • We used galactose to purify active proteins from a patient with FSGS • Proteins were separated on a gel. • A band of low molecular weight protein was present. • CLC-1 was the single cytokine identified in this material by mass spectrometry. Proteins of interest Savin VJ, ASN 2008 (abstract)
CLC-1 increases permeability and decreases expression of nephrin, the main junction protein Palb, CLC-1 * * * Rat glomeruli were treated with CLC-1 in various concentrations. CLC-1 increased permeability as does FSGS serum. Synthesis of nephrin, the main protein of the slit-junction, is decreased. * P< 0.01 vs C * Savin VJ, ASN 2008 (abstract)
Antibody to CLC-1 prevents permeability caused by patient serum or by CLC-1 itself Anti-CLC-1 mAb vs. without mAb: Fisher exact test, p < 0.02; paired t-test, p<0.005. Savin VJ, ASN 2008
Serum Urokinase Receptor and FSGS Wei et al, 2011
Summary of current work about circulating factor in FSGS • Permeability activity of plasma is highest in patients with severe disease. • Galactose binds the active protein and can be used for purification or for therapy. • CLC-1 is a candidate for the FSGS permeability factor • due to presence in FSGS plasma • same effects as FSGS plasma in vitro • suPAR
GALACTOSE: Case reports Case 1 NDT 2009; Cases 2 and 3 Therapeutic Apheresis Dial 2011
Galactose: Safety • IND #77,091 • 23 patients • Duration of therapy: 28 days • No SAE directly related to drug • AE: abdominal pain
Galactose: Dosing • Ferro Pfahnstiel, Inc. (Waukegan, IL) • Powder • 500 g in plastic container • Dose: 0.2 g/kg/dose BID (max: 15 g BID) • Dissolve in 15-30 mL water • Administer 15 minutes before breakfast and dinner
FONT Trial Study Summary * May be phone follow up
FONT Study Network 16 approved sites • Cohen Children’s Medical Center • University of Michigan • Cincinnati • Boston Children’s • University of Miami • University of Kansas • MUSC • Stollery • Emory • Oregon • Children’s Mercy • Texas Tech El Paso • Nationwide Children’s • Carolinas • Mayo Clinic • Columbia
Contact Information FONT2@umich.edu 1-855-4-FONTII (1-855-436-6844)